General Information about Benicar
As with any medication, Benicar could cause sure side effects, though not everybody experiences them. Common side effects could include dizziness, fatigue, headache, and nausea. More severe unwanted effects are rare however may embrace allergic reactions, issue respiration, chest pain, and swelling of the face, lips, or tongue. If you expertise any of those signs, it is important to seek medical consideration immediately.
Benicar is normally prescribed for adults and youngsters over the age of six who have been recognized with hypertension. It is out there in tablet type and is often taken as soon as a day. The dosage could range depending on the affected person's age, severity of hypertension, and other individual factors, and it should all the time be taken precisely as prescribed by a physician.
High blood strain is a standard condition affecting tens of millions of individuals worldwide, and if left untreated, it can enhance the danger of serious well being issues corresponding to heart disease, stroke, and kidney illness. Many elements can contribute to hypertension, together with genetics, lifestyle choices, and underlying medical circumstances. While way of life adjustments, similar to maintaining a wholesome weight, consuming a balanced diet, and exercising regularly, may help control blood stress, some individuals may have treatment to achieve adequate control.
There are also some precautions to focus on when taking Benicar. It just isn't recommended for pregnant or breastfeeding women or folks with a history of kidney disease or liver illness. Patients with a recognized allergy to olmesartan or different ARBs must also not take Benicar. Additionally, it is essential to inform your doctor of any other medications you're taking, including over-the-counter drugs and dietary supplements, to avoid potential interactions.
When taken often, Benicar helps to lower blood strain and stop problems related to high blood pressure. It can be utilized alone or in combination with other blood stress medicines, and the effectiveness of the therapy may be monitored by way of regular blood stress checks. In some cases, a affected person's dosage may need to be adjusted to attain the desired outcomes.
In conclusion, Benicar is a broadly used medicine for controlling high blood pressure in adults and kids. With its effectiveness in improving blood pressure and preventing related complications, it has turn out to be an essential a half of many sufferers' remedy plans. However, as with all medication, it is essential to observe your physician's directions, monitor for unwanted facet effects, and talk about any considerations or potential interactions with other medicine. By working intently along with your healthcare provider, you can successfully manage your blood stress and lead a healthier life.
Benicar, additionally identified by its generic name olmesartan, is a prescription medication generally used to deal with hypertension, or hypertension. It belongs to a class of medicine known as angiotensin II receptor blockers (ARBs), which work by blocking the action of a hormone called angiotensin II and helping blood vessels chill out and widen, thus lowering blood strain.
In uncommon cases, Benicar has been associated with a severe condition called sprue-like enteropathy, inflicting continual diarrhea and weight reduction. This side impact is extra widespread in individuals of Asian descent and those taking large doses of the medication. If you expertise persistent diarrhea or unexplained weight reduction, converse to your doctor instantly.
The impact of a neurointensivist on patients with stroke admitted to a neurosciences intensive care unit hypertension prevention buy benicar without a prescription. Improvement in intensive care unit outcomes in patients with subarachnoid hemorrhage after initiation of neurointensivist co-management. External ventricular drainage response in poor grade aneurysmal subarachnoid hemorrhage: effect on preoperative grading and prognosis. Cerebral arterial spasm- a controlled trial of nimodipine in patients with subarachnoid hemorrhage. Effect of different components of triple-H therapy on cerebral perfusion in patients with aneurysmal subarachnoid haemorrhage: A systematic review. Program Requirements for Advanced Training in Neurocritical Care: Neurological Surgery. Techniques and strategies in neurocritical care originating from southern Scandinavia. Weiss neurological examination should include evaluation of mental status, speech function and understanding, cranial nerve function (including that of the first cranial nerve), motor and sensory function, and reflexes, as well as cerebellar/gait testing. Of note, the sensory examination should include evaluation of proprioception and pinprick responses. Formal visual field and acuity examination may be required if there is concern for disease anywhere along the visual tracts, from the eye itself to the occipital lobe. Rectal examination for tone, volition, sensation, and the bulbocavernosus reflex is often required in evaluating spinal disease. Specific evaluation for surgical scars in the chest or abdomen may be valuable in the planning of a procedure that extends beyond the brain or spine, such as placement of a ventriculoperitoneal shunt. Computer documentation provides the surgeon with a useful tool for systemic and comprehensive evaluation of the history and physical examination findings. However, the surgeon must be deliberate, being cognizant of the potential for error when glossing over standard templates. Finally, many neurosurgical patients have significant comorbid conditions that necessitate evaluation preoperatively. Routine laboratory values, including a metabolic panel and blood cell count, are indicated before any nonemergency surgical procedure and should be obtained to screen for a number of underlying acute or chronic pathologic conditions that may pose a risk to a patient undergoing general anesthesia and surgery. The metabolic panel may suggest variations in sodium and potassium levels often noted in the neurosurgical patient population, as well as baseline renal function. Underlying anemia noted in the blood cell count must be investigated and corrected accordingly. Before definitive surgery, particular attention should be focused on platelet count, prothrombin time (international normalized ratio), partial thromboplastin time, and bleeding time (if necessary). Any suggestions of bleeding diathesis or coagulopathy should be further investigated and corrected. Many patients currently take anticoagulant or antiplatelet agents for a number of underlying medical comorbid conditions. Discontinuation or reversal of these agents (or perhaps initiation of these agents in selected endovascular cases) should be addressed at least 1 week before surgery. Blood typing and screening, or crossmatching for packed red blood cells and blood products, should be requested from the blood bank and verified in advance. A qualitative human chorionic gonadotropin level should be measured for every woman of childbearing age before surgery. Patients should undergo serum testing of a full or selective endocrine panel to evaluate any pituitary axis deficiencies. The thyroid and cortisol axes are uniquely critical, and abnormalities must be identified and corrected before any surgical procedure is performed. Ruling out nonsurgical lesions, such as prolactinomas, also necessitates judicious review of preoperative laboratory work. Comprehensive planning represents the first priority and foundation of any neurosurgical procedure. Because the nervous system has little tolerance for injury, the axiom "failing to prepare is preparing to fail" holds particularly true. This preparation begins with clear and careful definition of technical goals and potential pitfalls of each procedure. Effective planning then allows the necessary flexibility to manage deviations from a standard operative course. By taking the necessary steps to ensure adequate preparation for a case, the neurosurgeon may prevent or avoid many significant neurosurgical complications. The experience and ability to detect and handle the most adverse intraoperative events should therefore be a self-imposed limitation for any surgeon. Specifically, for an intervention in a disease process to be effective, the surgical team must understand the underlying pathophysiologic process or have a targeted plan to acquire further information. Unfortunately, even good patient selection and comprehensive planning cannot account for all anatomic and pathologic variables encountered during surgery. The surgeon must be amenable to potential alternative surgical goals upon encountering certain intraoperative findings or surgical pathology results. Surgical planning thereby seamlessly blends with a larger multimodal treatment plan to minimize morbidity and optimize timely diagnosis and treatment of disease. This chapter aims to provide a general framework to approaching a neurosurgical procedure, specifically focusing on essential considerations and supplemental measures necessary to provide a patient with an optimal outcome. Preoperative patient assessment regularly consists of a detailed and focused history, physical examination, and review of pertinent laboratory results and imaging studies. Disciplined, repetitive practice in these tasks allow for a comprehensive, detailed, and repeatable preoperative course that minimizes error. Subsequent delineation of time course and of onset of symptoms clarifies the degree of a suspected condition. In addition to establishment of pertinent positives, pertinent negatives should always be documented.
Gray matter astrocytes send processes to the pial surface blood pressure chart india cheap benicar uk, blood vessels, and nodes of Ranvier and therefore share many functions with white matter astrocytes. Gray matter contains less myelin and more vessels than white matter, so gray matter astrocytes perform these functions at different proportions. Astrocyte processes surround most synapses and, with the presynaptic terminal and the postsynaptic specialization, comprise the tripartite synapse. Astrocytic ensheathment of synapses helps inactivate and recycle neurotransmitters, such as the excitatory amino acid glutamate. The glutamate and other neurotransmitter transporters are highly enriched in astrocyte processes that ensheathe synapses. Intercellular calcium waves are also generated from astrocyte to astrocyte in response to neuronal stimulation. Gap junctions have been detected between astrocytes and neurons and, along with astrocytic neurotransmitter receptors, may couple astrocytic and neuronal physiology. One key to understanding this role Oligodendrocytes Rapid electrical communication among the 1011 neurons in the human brain controls and integrates the sophisticated mental and motor functions that set us apart from other species. Consider, for example, a complex task such as a 7-foot human dunking a basketball. The motor, sensory, and decision-making circuitry of the brain and peripheral nerves must integrate and coordinate jumping, manipulating the torso, handling the ball, avoiding defenders, and putting the ball in the basket. Millions of coordinated nerve impulses govern this action, and many must travel more than a meter in a fraction of a second. Without rapid nerve conduction, the 1011 neurons in the human brain would not be an advantage for function or survival. In invertebrates, axonal conduction velocity is related to the diameter of the axon. For example, the large-diameter motor axons conduct at a velocity of approximately 40 m/sec. If this conduction velocity were regulated solely by axonal diameter, the diameter of this axon would be several millimeters. Multiplying this by the millions of axons in the spinal cord would result in a spinal cord as wide as a telephone pole. Therefore an additional mechanism evolved to accommodate rapid nerve conduction in the vertebrate brain. One myelin internode is "unrolled" to depict continuity between oligodendrocytes and myelin internodes. The compact nature of myelin (m) is shown in the electron micrograph in the upper right. Myelin internodes end in paranodal loops at nodes of Ranvier, depicted in the cut-away view. Myelination supports saltatory conduction, in which ion exchange occurs only at the nodes of Ranvier (lower schematic). Along each axon, individual myelin internodes are separated from their neighbors by a node of Ranvier, a specialized unmyelinated axonal segment (1 to 5 µm in length) enriched in sodium channels and analogous to the axon hillock or initial axonal segment. The action potential "jumps" from node to node by a process called saltatory conduction. Myelin is essential for normal neurological function, and a variety of inherited, metabolic, and immune-mediated myelin diseases occur in humans. Axonal degeneration is a consistent and neurologically important phenotype in the brains of individuals with myelin disease,39 indicating that myelin provides extrinsic trophic support for the survival of axons. Therefore the distribution of oligodendrocytes correlates with the density of axons requiring myelin. Oligodendrocyte-myelin ratios, however, are not directly proportional, because different oligodendrocytes can myelinate different numbers of axons. As expected, oligodendrocyte density is high in white matter tracts, where the cells often occur in rows oriented parallel to axons. Oligodendrocytes are also present at significant densities in gray matter because many axons terminating on and originating from neurons are myelinated. Oligodendrocyte cell bodies can be found close to neuronal cell bodies in gray matter or close to blood vessels in both gray and white matter. Upper left schematic depicts unrolled myelin internode; the stippled area represents compact myelin (m), shown in the electron micrograph. The basal lamina forms a continuous tube around the entire length of each myelinated fiber. These Schwann cells have a molecular phenotype that differs significantly from myelinating Schwann cells. Because the entire adult mammalian brain is occupied by microglial cells, it is evident that they have functions that are specific to the brain. Historically, microglial cells were thought to originate from bone marrowderived monocytes. Although microglia share many characteristics with blood-borne monocytes, it is now established that microglia originate from a unique stem cell in the yolk sac. The proximal axon sprouts and uses the basal lamina (orange) as a substrate for regeneration (C). Neurons that lose this competition die; microglia do not kill these neurons, but they recognize their dysfunction or degeneration and remove them. Regional variations in the number and shape of microglia suggest that microglial distribution and morphology are regulated by local environments and that microglia play a role in tissue homeostasis. Although many aspects of this homeostasis remain to be elucidated, microglia respond quickly and dramatically to all forms of brain pathology. Intravital imaging of microglia revealed remarkable motility of microglial processes under normal physiologic conditions. Microglial function in the normal brain is better described as one of surveillance.
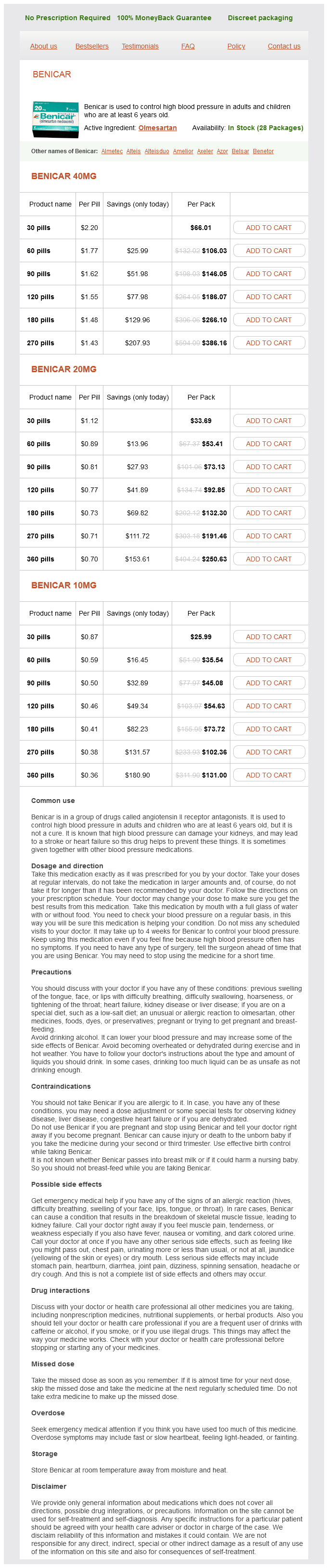
Benicar Dosage and Price
Benicar 40mg
- 30 pills - $66.01
- 60 pills - $106.03
- 90 pills - $146.05
- 120 pills - $186.07
- 180 pills - $266.10
- 270 pills - $386.16
Benicar 20mg
- 30 pills - $33.69
- 60 pills - $53.41
- 90 pills - $73.13
- 120 pills - $92.85
- 180 pills - $132.30
- 270 pills - $191.46
- 360 pills - $250.63
Benicar 10mg
- 30 pills - $25.99
- 60 pills - $35.54
- 90 pills - $45.08
- 120 pills - $54.63
- 180 pills - $73.72
- 270 pills - $102.36
- 360 pills - $131.00
Rapid diagnosis of meningitis is critical for early initiation of appropriate treatment and has a direct effect on patient outcome; hence the salient features of laboratory work-up are also covered blood pressure medication gives me a headache benicar 40 mg purchase on-line. In addition to bacterial and other infections, this chapter covers aseptic meningitis and encephalitis, that is, inflammatory conditions affecting these structures that are not caused by an easily identifiable infectious agent. The multiple infectious etiologies associated with aseptic central nervous system inflammation include viruses, fungi, parasites, protozoa, and Rickettsia species. The epidemiology, transmission, clinical features, and treatment of meningitis and encephalitis caused by these entities are presented in detail. The leak persisted over the next 9 months, during which time she suffered three separate bouts of meningitis, the first of which was culturepositive for Streptococcus intermedius. This axial T1-weighted magnetic resonance image, with contrast administration, was obtained during the third episode. It shows diffuse enhancement over the brain convexities and falx cerebri, a classic finding in active bacterial meningitis. Of note, the frontal sinus shows mucosal thickening and enhancement consistent with paranasal sinusitis. McCutcheon 40 Meningitis is defined as inflammation of the meninges, the lining of the brain and spinal cord. The typical symptoms, headache and fever, are each shared by several other diseases, and thus the diagnosis of meningitis requires a high index of suspicion and ultimately the definitive diagnostic test-a lumbar puncture. Bacterial meningitis may be community-acquired or hospital-acquired (nosocomial), each with its own associated pathogens. Even with advances in antibiotic therapy, meningitis remains a serious disease that can result in significant morbidity and mortality. Recurrent bacterial meningitis is a unique and therapeutically challenging condition that will also be covered in the bacterial meningitis section of this chapter. Nonbacterial (aseptic) forms of meningitis can produce clinical syndromes that overlap those of infectious meningitis; they also are considered in this chapter. Encephalitis represents inflammation of the brain, and the pathogens typically responsible are quite different from those usually seen in meningitis; the overlap between the two (meningoencephalitis) is also possible and is addressed here as well. Ventriculitis is focal or diffuse inflammation of the ependymal lining of the cerebral ventricular system. It has no specific clinical syndrome to distinguish it from meningitis, and a diffuse encephalitis usually reaches the ependyma. BacterialPathogens Table 40-1 lists the common pathogens in bacterial meningitis by age and risk factors. Streptococcus pneumoniae remains the leading cause of bacterial meningitis in the United States. Additionally, up to 60% of patients with the disease have a nidus of infection such as otitis, sinusitis, or endocarditis. Pneumococcal vaccines have been developed and proved to be very effective in the prevention of invasive pneumococcal disease, including meningitis. The efficacy of the heptavalent pneumococcal conjugate vaccine (approved in the United States in 2000) has been reported to be as high as 97%. Specifically, the incidence decreased by 64% for patients younger than 2 years, and by 54% for patients 65 years and older, during the study period. Neisseria meningitidis is a common cause of meningitis in young adults and children (after the neonatal period). It is a life-threatening condition and a source of significant morbidity and mortality, with 30% to 50% of survivors sustaining neurological sequelae. For example, a populationbased surveillance study of all the acute-care hospitals in four U. The classic meningitis triad-fever, neck stiffness, and altered mental status-is reportedly present in only 27% of patients with meningococcal meningitis. Current guidelines for meningococcal meningitis recommend the use of penicillin or ampicillin. Predisposing conditions for meningitis include diabetes mellitus, asplenic states, alcoholism, and immunodeficiency. Traditionally, individuals living in close quarters, such as military personnel and college students in dormitories, are considered at moderately higher risk for meningococcal meningitis. Meningococcal disease has also been associated with smoking and with deficiencies in the complement system, specifically the terminal components (C5 through C8 and possibly C9). Listeria monocytogenes is responsible for 2% of bacterial meningitis cases in the United States. It is the responsible pathogen in 20% of cases of bacterial meningitis in both neonates and adults older than 50 years. These patients have a longer duration of symptoms prior to presentation than those with meningitis due to other pathogens. This bacterium has been isolated from vaginal and rectal cultures in 15% to 35% of asymptomatic pregnant women. The child of an infected mother is infected through vertical transmission during delivery. Such risk factors include advanced age (>60 years), diabetes, liver or kidney failure, pregnancy or postpartum condition, malignancy, and collagen vascular disease. The development of bacterial meningitis depends on the following steps of bacterial-host interaction: 1. Neuronal injury Most cases of meningitis occur from hematogenous spread or by direct extension from bacterially colonized cranial structures adjacent to the meninges.