General Information about Bimat
Apart from its therapeutic makes use of, Bimat has gained reputation in the cosmetic world as nicely. Women all around the world need lengthy and thick eyelashes, as they are thought of a logo of magnificence. Bimat has proved to be a game-changer for those who have skinny or sparse eyelashes, because it helps in lengthening and thickening them. It works by growing the expansion section of the eyelash hair and making the lashes appear longer and fuller. Bimat for cosmetic use can be out there within the form of an eyelash serum that's applied every day to the bottom of the upper eyelashes.
In conclusion, Bimat has revolutionized the therapy of glaucoma, ocular hypertension, and beauty enhancement of eyelashes. Its effectiveness and minimal side effects have made it a preferred selection amongst sufferers and healthcare professionals. Proper use of this medicine can help in stopping vision loss and reaching beautiful, long eyelashes. However, it is always advisable to consult a doctor before using Bimat to make sure its protected and effective use. Remember, healthy eyes are a present and it is our accountability to deal with them.
Bimat is a secure and effective treatment when used as directed by a healthcare skilled. However, as with every medicine, there could also be some unwanted effects, corresponding to mild irritation or redness in the eye, darkening of the pores and skin across the eye, and elevated size and thickness of eyelashes. These unwanted effects are usually gentle and resolve on their own. It is essential to follow the dosing instructions and precautions as prescribed by the physician to attenuate the chance of unwanted facet effects.
Eyes are considered to be the window to the world and it's important to take good care of them. In recent times, eye problems have turn into a typical well being downside. One such disorder is glaucoma, which is a leading explanation for blindness worldwide. In addition, many individuals also undergo from ocular hypertension, a condition in which the pressure inside the attention is higher than normal. These eye situations require proper remedy to prevent any injury to the optic nerve and preserve good imaginative and prescient. One of the most effective and extensively used therapies for these eye issues is Bimat.
Bimat: A Breakthrough in Eye Care Treatment
Ocular hypertension is another condition by which the pressure inside the eye is higher than regular however doesn't trigger any injury to the optic nerve or imaginative and prescient loss. If left untreated, it could finally result in glaucoma. Bimat can additionally be used in the remedy of ocular hypertension to scale back the pressure inside the attention and prevent any future problems.
Glaucoma is a condition by which stress builds up inside the eye, damaging the optic nerve and causing imaginative and prescient loss. If left untreated, it may possibly ultimately result in blindness. Bimat helps in decreasing the stress inside the eye by growing the flow of fluid out of the attention, thereby stopping any further damage to the optic nerve. It is available in eye drop type and is usually applied once a day in the affected eye. Bimat has been proven to be extremely effective in lowering intraocular stress and preventing any progression of glaucoma.
Bimat, additionally identified by its generic name bimatoprost, is a medication used for the remedy of glaucoma, ocular hypertension, and lengthening eyelashes. It belongs to the category of medicines known as prostaglandin analogs and works by lowering the stress inside the eye. Bimat was first permitted by the Food and Drug Administration (FDA) in 2001 for the remedy of glaucoma and ocular hypertension. However, in latest times, it has additionally gained popularity for its cosmetic use in lengthening and thickening eyelashes.
In most of the reported cases from India symptoms migraine buy genuine bimat on-line, history of tuberculosis in the past or during detection was noted. The mechanism of the bleeding is unknown; it has been attributed to friction between the fungus ball and the hypervascular wall, to endotoxins liberated from the fungus, and to a type 3 reaction in the cavity wall. Because most of the pre-existing cavities are due to tuberculosis, mycetomas are most often found in the upper lobes or in the superior segment of the lower lobes. The air crescent sign is not specific to mycetoma formation, it can also be seen in patients with blood clot within a pre-existing cavity, necrotic carcinoma, ruptured hydatid cyst and lung abscess with necrosis. If the fungus ball completely fills the cavity, the air crescent may not be observed. Mobility can be readily demonstrated by turning the patient although it is rarely necessary as the diagnosis is obvious in most cases. The characteristic chest radiographic findings include central bronchiectasis and mucoid impaction seen typically as branching opacities, usually central and in an upper lobe distribution-the "gloved finger sign" These. It is seen on chest radiographs as a ground glass opacity and/or diffuse small nodules. Sometimes recurrent transient opacities superimposed on a fine micronodular pattern may be seen. Chronic hypersensitivity pneumonitis typically presents as traction bronchiectasis and interstitial thickening often associated with areas of ground-glass opacity and mosaic perfusion. Many patients with cryptococcal pneumonia have no symptoms and the pulmonary lesions seen radiographically heal spontaneously. Fortunately, they are not commonly found in the Indian subcontinent and are natural inhabitants of North and South America. These include species like Histoplasma, Coccidioides, Blastomyces, and Paracoccidioides. In both there is necrosis of pulmonary tissue followed by fibrosis and contraction. Other manifestations can be pulmonary granulomas or small nodules scattered in both lung fields resembling military tuberculosis. Although it can occur as pulmonary or disseminated disease in otherwise normal individuals, cryptococcosis is more frequently seen to affect immunocompromised patients. In the immunocompetent individuals, the radiographic findings can be single or multiple pulmonary nodules or areas of segmental 2560 Section 6 Chest and Cardiovascular Imaging Coccidioidomycosis It is caused by the fungus Coccidioides immitis and found principally in endemic areas in southwestern United States and northern Mexico the most common radiological manifestation of primary coccidioidomycosis is a single or multiple foci of airspace consolidation. Thin walled cavities, pleural effusion and mediastinal lymphadenopathy may rarely be seen. Those whose symptoms or radiographic abnormalities remain after 68 weeks are considered to have chronic pulmonary coccidioidomycosis. The radiologic manifestations include lung nodules and cavities and rarely bronchiectasis and scarring. Apical fibrocavitary disease with lobar contraction, bronchiectasis and rarely calcification may resemble reactivation tuberculosis. If the abscess ruptures through the diaphragm, basal consolidation with cavitation may be seen. Metazoal Infestations Roundworm, Hookworm and Strongyloides Infections Many parasitic worms, including Ascaris, Taenia, Ankylostoma, and Strongyloides pass through the lungs as part of their life cycle. In most instances, no pulmonary complications occur with any of these worms, but in a few patients, an allergic reaction takes place in the lung parenchyma, which manifests itself radiographically as dense migratory pulmonary consolidations without recognizable segmental distribution. Changes can occur at the base of either lung, because of the relationship of the liver to the diaphragm, but are much more frequent on the right. An amebic liver abscess may extend through the diaphragm into the pleural cavity, giving rise to an empyema. It can cause tropical eosino-philia, a syndrome consisting of cough, wheezing and severe blood eosinophilia. This is believed to be due to an immunologic response to the microfilariae rather than to a direct infection. Humans are accidental hosts and acquire infection by ingesting ova from fomites or contaminated water and by direct contact with dogs. Larvae develop in the duodenum of the host, enter the bloodstream and travel to the endorgans. Disease results from the cysts that develop around this parasite in the endorgans. The cyst wall consists of 3 layers: an outermost layer is the pericyst which is a fibrotic capsule formed by the compression of the adjacent lung tissue. The cyst itself has a thin wall composed of 2 adherent layers, an outer ectocyst and an inner delicate lining-the endocyst. Multiple cysts are seen in approximately one third of patients and are bilateral in 20%. The internal contents are of water density and daughter cysts when present, are seen as curved septations within the main cyst. The cysts are relatively pliant and mold to adjacent structures, resulting in indentation, lobulation ar flattening. Calcification, which is a common feature of hydatids in the liver, is very rare in lung cysts. If the pericyst ruptures, with the two inner layers remaining intact, air dissects between the pericyst and ectocyst giving rise to a crescent or meniscus sign. Rupture into the pleural space causes an effusion or if there is an additional airway communication, a hydropneumothorax. Hydropneumothorax the appearance of gas in the pleural space together with fluid is usually iatrogenic in origin. It may be associated with a bronchopleural fistula casued by rupture of a pneumatocele or abscess, and is seen particularly with S. In approximately 510% of patients, however, parapneumonic effusion progresses to frank intrapleural pus.
Many also forgo recommended cancer screenings for secondary malignant neoplasms and follow-up surveillance medications that cause hyponatremia order bimat 3 ml visa. This section will focus on several lifestyle-related changes that are important for cancer survivors. Immunizations and prevention of infections are also important and are addressed in a different chapter. Secondary Malignant Neoplasms Infertility is a potential health problem among cancer survivors because many cancer survivors are of childbearing age. Before cancer treatment, the risks of infertility post-cancer treatment should be discussed with patients, and health care providers should evaluate whether fertility preservation could be an option for these patients. In women, one common consequence of treatment for breast cancer is hormonal depletion, which may result in premature menopause. Among patients receiving doxorubicin and cyclophosphamide followed by docetaxel, the incidence of amenorrhea was 54. Several strategies, including embryo or oocyte cryopreservation and conservative gynecologic surgery, can preserve fertility in females. Men should be advised of a potentially higher risk of genetic damage to sperm collected after chemotherapy. In addition to cytotoxic chemotherapy, recipients of targeted therapies such as bevacizumab may have an increased risk of ovarian failure. The manufacturer of bevacizumab states that providers should inform women who are of reproductive potential about the risk of ovarian failure before beginning bevacizumab treatment. In addition, survivors receiving tyrosine kinase inhibitors (imatinib, dasatinib, and nilotinib), thalidomide, and lenalidomide should be aware that these agents are teratogenic in animal models and/or humans. In one report, women who conceived while using imatinib had reported abnormalities and complex malformations, which are clearly of concern. Current recommendations do not favor continuing tyrosine kinase inhibitor therapy during pregnancy. Because the overall cancer rate is higher among survivors than among the general population, it is crucial that survivorship care incorporate screening and early detection for secondary primary cancers. In the United States, about 18% of all malignancies are a second (or subsequent) cancer (Howlader 2016). Having several risk factors may contribute to the onset of second cancers, including genetic susceptibilities, shared causative factors. The American Cancer Society has provided specific recommendations for adult survivors of several cancers, which are summarized in Box 1-1. Lifestyle-Related Prevention Exercise Obesity and low levels of physical activity are associated with higher risks of cancer recurrence and mortality. Studies have also suggested that weight gain after cancer diagnosis is associated with a higher risk of recurrence. Healthy lifestyle habits such as engaging in routine physical activity and maintaining a healthy diet and weight improve health outcomes and quality of life. Survivors should routinely be assessed for their readiness to participate in physical activity and the level of physical activity in which they engage. Common barriers to physical activities include having inadequate time to exercise, lacking access to an exercise environment, having a lack of safety knowledge for exercise, having a lack of knowledge of appropriate exercise activities, and having physical limitations that result from symptoms. American Cancer Society/American Society of Clinical Oncology breast cancer survivorship care guideline. All survivors should be encouraged to avoid inactivity or a sedentary lifestyle and return to daily activity as soon as possible. All survivors are recommended to engage in a moderate level of physical activity after cancer treatment. Breast cancer survivors with lymphedema should also consider meeting with an exercise specialist before initiating upper-body strength training exercise. Weight and Nutrition Management Weight management is essential among cancer survivors. Obesity is a risk factor for postoperative complications, secondary cancer, cancer recurrence, and development of diabetes. Strategies for weight management should be discussed to prevent weight gain for normal and overweight survivors/ survivors with obesity. Clinicians should discuss portion control and refer overweight survivors/survivors with obesity to dietitians for weight management. Strategies for weight loss such as medications or bariatric surgery are not well studied among cancer survivors. Survivors should be encouraged to make informed choices about food to ensure variety and an adequate nutrient intake. Current recommendations suggest that survivors maintain a dietary pattern that is high in vegetables, fruits, and whole grains and legumes; low in saturated fats; and limited in alcohol consumption. Smoking Cessation Despite all the known health risks associated with smoking, an American Cancer Society survey found that about 10% of all cancer survivors are smokers, with smoking prevalence highest among survivors of bladder, lung, and ovarian cancers (Westmaas 2014). In addition, according to the National Health and Nutrition Examination Survey, 64% of all cancer survivors who regularly smoked before their cancer diagnosis continue to smoke (Tseng 2012). Several characteristics, such as being female, of young age, and Hispanic, were identified for continued smoking after cancer treatment. Studies have also identified barriers that impede patients with cancer and cancer survivors from smoking cessation. These factors include stress, dependence, environmental factors, lack of resources, lack of support for quitting, and life challenges that result from their cancer diagnosis.
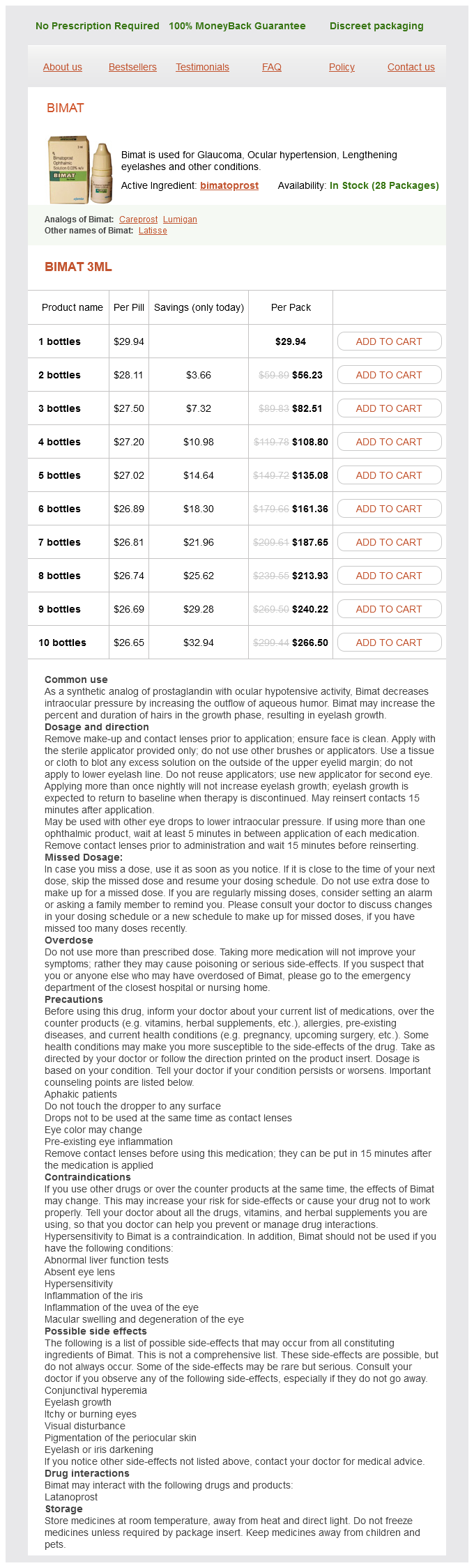
Bimat Dosage and Price
Bimat 3ml
- 1 bottles - $29.94
- 2 bottles - $56.23
- 3 bottles - $82.51
- 4 bottles - $108.80
- 5 bottles - $135.08
- 6 bottles - $161.36
- 7 bottles - $187.65
- 8 bottles - $213.93
- 9 bottles - $240.22
- 10 bottles - $266.50
Associated peripheral parenchymal distortion is common with paracicatricial emphysema treatment ulcerative colitis order cheap bimat on-line. At imaging, coal-worker pneumoconiosis and silicosis are similar, and the two diseases have features that overlap. The radiographic pattern of simple coal-worker pneumoconiosis include small round ill-defined/granular nodules, ranging 15 mm. Proliferation around bronchioles leads to distal air trapping and aircyst formation. It is restricted to women of childbearing age, and is not associated with smoking. Progressive dyspnea, spontaneous pneumothorax, chylothorax and hemoptysis are frequent clinical manifestations of the disease. Extrapulmonary manifestations include thoracic and abdominal lymphadenopathy, chylous ascites, pericardial effusion, renal angiomyolipomas, and lymphan-giomatosis. A bilateral, symmetrical reticular pattern is seen involving all lung zones to a similar degree (80%) or the lower zones predominantly in the remaining 20% patients. Involvement of the lymphatics may cause obstruction and accumulation of chylous pleural effusions in 1020%. Recurrent pneumothoraces are frequent (3040%), due to spontaneous rupture of these thin-walled cysts. Frontal chest radiograph shows large, parahilar fibrotic masses with surrounding cicatricial emphysema. With time, there is a progression from cellular nodules to fibrotic nodules forming stellate peribronchiolar scars. Smoking cessation is essential and leads to stabilization of symptoms in most patients. Chemotherapeutic agents, such as vinblastine, methotrexate, and cyclophosphamide have been used in patients with progressive disease unresponsive to corticosteroids or with multiorgan involvement. These cysts measure between 2 mm and 2 cm in diameter and are uniformly distributed throughout the lungs. The wall thickness of the cysts ranges from rarely perceptible to few millimeters. Extrapulmonary manifestations may occur in 515% of patients and include bone lesions, diabetes insipidus, and skin lesions. Constitutional symptoms, such as weight loss, fever, night sweats, and anorexia, occur in up to one-third of patients. Chest radiographs demonstrate nodular or reticulonodular opacities predominantly in the upper lungs. As the disease advances, cystic changes and bullae appear in the upper lungs and lung volumes increase. Early in the disease, nodules of 15 mm diameter predominate, mainly in a peribronchiolar (centrilobular) distribution. Rupture of cysts in the pleural space is the cause of the frequent episodes of pneumothorax. Approximately 50% of patients experience a favorable outcome with partial or complete clearing of radiologic abnormalities and symptom resolution. In 1020%, recurrent pneumothorax or progressive respiratory failure with cor pulmonale occurs. The typical radiograph reveals bilateral central and symmetric lung opacities, with relative sparing of the apices and costophrenic angles. Less commonly, radiographs show multifocal asymmetric opacities or extensive diffuse consolidation without any clear zonal predominance. Opacities range from a groundglass appearance with indistinct margins, to reticular or reticulonodular, to consolidation with air bronchograms. Imaging Features the chest radiograph is normal in most patients with early disease. In patients who have mild disease, the findings usually consist of symmetrical, basal, fine reticular opacities. As the disease progresses, the abnormalities become more diffuse and assume a coarser reticular pattern. However, histological confirmation should be obtained in all patients with atypical imaging findings, such as extensive ground-glass opacities, nodules, consolidation, or a predominantly peribronchovascular distribution. The term idiopathic is reserved for those conditions in which the cause of the lung injury pattern is unknown. The classification was published in full in the American Journal of Respiratory and Critical Care Medicine in 2002. In addition to the temporal heterogeneity, the histological abnormality is spatially heterogeneous, with patchy lung involvement and normal lung adjacent to severely fibrotic lung. Patients present with gradually worsening dyspnea over several months, and they often experience fatigue and weight loss. Imaging Features the radiographic manifestations are heterogeneous and range from predominantly reticular pattern to mixed reticular and airspace patterns. Less common findings include areas of consolidation, honeycombing and centrilobular nodules. Women and men are equally affected and present with mild dyspnea, cough, and fever that have been developing over a few weeks. There is no association with cigarette smoking;in fact, most patients are nonsmokers or ex-smokers. The majority of patients recover completely after administration of corticosteroids, but relapses occur frequently within 3 months after corticosteroid therapy is reduced or stopped.