General Information about Celebrex
Celebrex can additionally be a most well-liked choice for many individuals as a outcome of its convenience and ease of use. It is on the market in capsule type, which may be taken a few times a day relying on the severity of ache and the individual's response to the medicine. Unlike different NSAIDs which will have to be taken a quantity of occasions a day, Celebrex's longer period of action implies that it can present continued relief without the need for frequent dosing.
Like any treatment, Celebrex could cause unwanted side effects in some people. These can vary from gentle to extreme depending on the particular person's medical historical past and other drugs they may be taking. Some frequent unwanted effects embrace headache, dizziness, abdomen upset, and pores and skin rash. More severe unwanted effects, though uncommon, might embrace allergic reactions, liver damage, and an increased risk of coronary heart assault and stroke.
One of the primary benefits of Celebrex is its capability to focus on the COX-2 enzyme, which is answerable for inflammation and pain. Unlike its predecessor, Vioxx, which was pulled from the market within the early 2000s due to its link to an increased risk of heart attack and stroke, Celebrex has been proven to be a safer alternative. This is as a result of it additionally inhibits COX-1, another enzyme that performs a role in blood clotting and defending the lining of the stomach. This balanced inhibition of each COX enzymes makes Celebrex less likely to trigger severe opposed results on the center and stomach.
It is important to tell your physician of some other medicines or supplements you take before starting Celebrex, as it could work together with certain medication. People with a history of heart disease, hypertension, or abdomen ulcers should also train caution and inform their physician earlier than beginning this medicine.
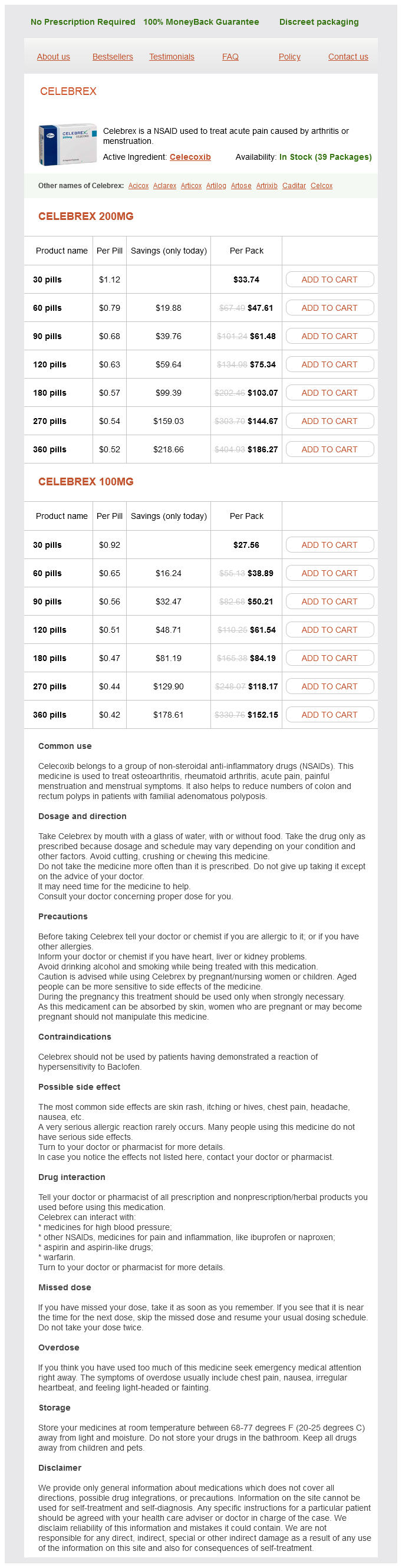
Celebrex, additionally known by its generic name celecoxib, is a non-steroidal anti-inflammatory drug (NSAID) that's commonly used to treat acute pain attributable to circumstances such as arthritis and menstruation. It is a prescription medicine that works by decreasing the hormones in the physique that cause irritation and pain.
For these suffering from arthritis, whether or not or not it's osteoarthritis or rheumatoid arthritis, the ache, stiffness, and swelling can greatly influence daily actions and quality of life. This is where Celebrex comes in, offering reduction and enhancing total function for those battling this continual illness.
In conclusion, Celebrex is a commonly used NSAID that provides efficient reduction for acute ache attributable to arthritis and menstruation. Its unique ability to focus on inflammation whereas additionally protecting the abdomen lining and stopping blood clotting makes it a safer various to other NSAIDs. However, as with every treatment, you will want to use it under the steerage of a healthcare skilled and to be aware of potential unwanted facet effects.
It is essential to note, nevertheless, that while Celebrex offers efficient ache aid, it is not a cure for arthritis or some other condition. It merely supplies short-term relief and does not handle the underlying explanation for the pain. Therefore, it shouldn't be used as a long-term therapy choice and may always be taken underneath the supervision of a healthcare professional.
Menstrual cramps, also referred to as dysmenorrhea, may be debilitating for some girls and may greatly impression their every day actions and productiveness. Celebrex is also a generally used remedy option for this type of acute ache. As with arthritis, it targets the COX enzymes to reduce the manufacturing of prostaglandins, which are responsible for the uncomfortable symptoms associated with menstrual cramps.
The aim of cleft surgery is the restoration of normal anatomy and the promotion of normal growth and development of all structures affected by the cleft gouty arthritis in back order 100 mg celebrex with amex. Emphasis must be placed on the restoration of muscle continuity whether of the lip and/or nose, or the soft palate. Techniques in which these concepts are promoted have been shown to produce the most acceptable results in the long-term. In reality, given even the most favourable circumstances, secondary surgery may be required and a return to the basic principles employed in primary surgery rather than modifying the existing state is necessary. However, there are other surgical procedures that are required as the child grows older. Where problems with speech exist, that cannot be resolved by therapy alone, velopharyngeal surgery may be necessary. Following assessment, this includes revision palatoplasty, palatal lengthening or pharyngoplasty. Later, in clefts involving the alveolus, bone grafting is carried out usually between the ages of 7 and 11 years. When growth is complete orthognathic surgery to correct abnormal facial bone development, in particular an under-developed maxilla, may be needed. Finally, there may be residual deformities of the nose and rhinoplasty will be required. Ultimately, the adherence to an agreed protocol working in a fully equipped and co-ordinated setting with a full complement of concerned professionals and the facility for collection of data such that problems can be identified and corrected at the earliest possible opportunity, will enable the surgeon to ensure the best outcome. Craniofacial Surgery Craniofacial surgery is concerned with the management of patients presenting with congenital or acquired conditions, affecting the hard and soft tissues of the head and face. The Department of Health approves and funds designated centres for the management of craniofacial conditions including: Craniosynostoses Craniofacial dysostoses Orbital dysostosis Encephalocoeles Craniofacial clefts these conditions are evident early in life and most patients are children under the age of 2. Patients referred to designated units are assessed and investigated by a multidisciplinary team and treatment combines the principles of maxillofacial reconstruction with neurosurgery. The surgical techniques employed in congenital conditions can also be applied to good effect in the treatment of skull base tumours and craniofacial trauma. Premature fusion of one or more skull sutures (craniosynostosis) occurs in 1 in 2,000 of the population. Syndromic craniosynostoses, such as Crouzon and Apert syndromes occur in 1 in 10,000 and 1 in 150,000 live births respectively. Historically, patients underwent numerous procedures performed by various clinicians from different surgical specialties. Results were generally poor and associated with high morbidity and even mortality. Many patients with severe deformity were denied surgery, because of the risks involved. The surgery is major, often protracted and associated with significant blood loss in the small child. Intensive care is needed for the more complex cases, or where the airway is compromised. Some children require more than one procedure as growth and dental development influence facial form and function. However, with an active, established team and utilising contemporary techniques, such as distraction osteogenesis, it is possible to perform fewer, more extensive procedures. The craniofacial principles of wide surgical exposure, primary bone grafting and internal fixation should be applied to the management of complex craniofacial trauma. Severely injured patients of all ages can be stabilised and offered early definitive treatment using these techniques. Morbidity is reduced and hospital stay shortened and there is an overall improvement in outcome. These surgical approaches can also be used to access intracranial and skull base lesions. By drawing on expertise gained in the management of trauma, tumour and congenital disease of the soft and hard tissues of the face, the maxillofacial surgeon plays a key role in craniofacial surgery. Skull Base Surgery the base of the skull is a complex and relatively inaccessible region. Pathology in this area may arise from either within the skull itself or from adjacent areas such as the paranasal sinuses, the orbit and the face. Conventional approaches to skull base lesions frequently require prolonged retraction of the brain and/or the resection of uninvolved structures to improve exposure. The resultant morbidity of such techniques, in terms of both cerebral function and facial appearance were often considerable with the result that many deep-seated skull based tumours were considered inoperable. The limited access also made adequate reconstruction of defects difficult and, in some cases, impossible. Recent developments in surgical approaches to the skull base are based on the temporary disarticulation or dismantling of the skeleton of the face and the skull to varying degrees. These bone segments are mobilised either as free bone segments, completely detached from the soft tissues, or pedicled to the soft tissues to retain their blood supply. In most cases the so-called "access osteotomy" is combined with a conventional craniotomy. Facial incisions are avoided wherever possible - the coronal scalp flap and intraoral incisions providing adequate exposure in many cases. If facial incisions are necessary, these are carefully sited and will usually heal with an imperceptible scar. Maxillofacial Surgeons, by virtue of their training in surgery of the facial bones and soft tissues, have contributed significantly to the development of the surgical access techniques now in common practice.
Also arthritis in the knee pictures cheap 200 mg celebrex fast delivery, it should be borne in mind that CerK expression may not be the same in all cell types. The relevance of CerK in cell biology was also highlighted in studies using CerK null mice; specifically, a potent reduction in the amount of neutrophils in the blood and spleen of these animals compared to their wild type counterparts was observed, whereas de amount of leukocytes, other than neutrophils, was increased in those mice. These observations suggested an important role of CerK in neutrophil biology (Graf et al. Therefore, the role of this protein in cell biology is unclear at the present time. CerK has also been reported to exist in dicotyledonous plants, where it was associated to the regulation of cell survival (Bi et al. Also, it has been recently found that a conserved cystein motif is critical for rice CerK activity and function (Bi et al. However, no reports on the possible existence of Cerk in monocot plants are available at the present time. Catabolism of ceramide 1-phosphate From the above discussion, it should be apparent that C1P is a bioactive metabolite, capable of altering cell metabolism rapidly and potently. So, the existence of enzymes capable of degrading C1P seemed to be feasible for regulation of C1P levels. Dephosphorylation of C1P might be a way of terminating its regulatory effects, although the resulting formation of ceramide could potentially be detrimental for cells. It could be speculated that another possibility for degradation of C1P might be its deacylation to S1P, which could then be cleaved by lyase activity to render a fatty aldehyde and ethanolamine phosphate (Merrill & Jones, 1990), or to Role of Ceramide 1-Phosphate in the Regulation of Cell Survival and Inflammation 405 sphingosine by the action of S1P phosphatases. However, no C1P deacylases or lyases have so far been identified in mammalian tissues, suggesting that the only pathway for degradation of C1P in mammals is through phosphatase activity. Ceramide 1-phosphate and the control of cell growth and death the first report showing that C1P was biologically active was published in 1995 (GomezMunoz et al. Activation of this kinase was tested my measuring the phosphorylation state of its downstream target p70S6K after treatment with C1P. Concerning intracellular calcium levels, which have also been implicated in the regulation of cell proliferation, the situation is controversial. Finally, it should be pointed out that C1P has been recently shown to be a key mediator in the development and survival of retina photoreceptors, and to also play a critical role in photoreceptor differentiation (Miranda et al. We previously demonstrated that natural C1P blocked apoptosis in bone marrow-derived macrophages (Gomez-Munoz et al. Also, downregulation of CerK blocked epithelial growth factor-induced cell proliferation. However, in contrast to these observations, it was reported that addition of the cell-permeable C2-ceramide to cells overexpressing CerK led to C2-C1P formation and stimulation of apoptosis (Graf et al. This controversy can be explained by the fact that overexpression of CerK would substantially increase the intracellular levels of C1P, especially when cells are supplied with high concentrations of exogenous cell permeable C2-ceramide; this action would cause overproduction of C2-C1P inside the cells, which is toxic at high concentrations (GomezMunoz et al. When cells become apoptotic, their metabolism undergoes important changes from early stages. This suggested the intervention of a different pathway for ceramide generation in these cells. The prosurvival effect of C1P was highlighted by the demonstration that intracellular levels of C1P were substantially decreased when the cells became apoptotic. Once generated, ceramides act on different intracellular targets to induce apoptosis. As mentioned above, C1P can be metabolized to ceramide by different phosphatases, and then further converted to sphingosine and S1P by the coordinated actions of ceramidases and sphingosine kinases. Therefore, it could be speculated that the effects of C1P might be mediated through C1P-derived metabolites. Therefore, it can be concluded that C1P acts on its own right to regulate cell homeostasis. The above observations suggest that regulation of the enzyme activities involved in ceramide and C1P metabolism is essential for cell fate. Elucidation of the mechanisms controlling ceramide and C1P levels may help develop new molecular strategies for preventing metabolic disorders, or designing novel therapeutic agents for treatment of disease. Ceramide 1-phosphate and the control of inflammation Inflammation is, in principle, a beneficial process for protecting the organism against infection or injury. Apart from the classical signaling pathways and metabolites that are involved in the regulation of 408 Biochemistry inflammation, it is now well accepted that ceramides are key elements in the inflammatory response (Lamour & Chalfant, 2005; Wijesinghe et al. Inflammatory mediators include chemokines, cytokines, vasoactive amines, products of proteolytic cascades, phospholipases, or lipids such as eicosanoids and sphingolipids. Sphingolipids, including ceramides, have also been described as key mediators of inflammation (Hayakawa et al. More recently a role for ceramide in the development of allergic asthmatic responses and airway inflammation was established (Masini et al. Subsequently, it was proposed that at least some of the proinflammatory effects of ceramides might in fact be mediated by its further metabolite C1P. It was concluded that the biological activity of C2-C1P does not occur via eicosanoid synthesis (Wijesinghe et al. Also, C1P was shown to act in coordination with S1P to ensure maximal production of prostaglandins. Further details on the role of C1P in inflammatory response can be found in different reviews (Chalfant & Spiegel, 2005; Lamour et al. Ceramide 1-phosphate and the control of cell migration Macrophage populations in tissues are determined by the rates of recruitment of monocytes from the bloodstream into the tissue, the rates of macrophage proliferation and apoptosis, and the rate of macrophage migration or efflux. Recently, our group demonstrated that exogenous addition of C1P to cultured Raw 264. Interestingly, this action could only be observed when C1P was applied to the cells exogenously, and not by increasing the intracellular levels of C1P.
Celebrex Dosage and Price
Celebrex 200mg
- 30 pills - $33.74
- 60 pills - $47.61
- 90 pills - $61.48
- 120 pills - $75.34
- 180 pills - $103.07
- 270 pills - $144.67
- 360 pills - $186.27
Celebrex 100mg
- 30 pills - $27.56
- 60 pills - $38.89
- 90 pills - $50.21
- 120 pills - $61.54
- 180 pills - $84.19
- 270 pills - $118.17
- 360 pills - $152.15
Frequent monitoring of uric acid arthritis pain feet order 100 mg celebrex amex, electrolytes, liver function, and coagulation profile was performed during the first 34 weeks of induction. Chromosome analysis revealed a normal male karyotype, confirming hematological and cytogenetic remission. This patient should be treated using standard induction therapy with steroids, vincristine, anthracycline, and cyclophosphamide (7,8). High-dose methotrexate should be used with caution and may require dose reduction. Similar to pediatric patients, hypersensitivity, pancreatitis, thrombosis, and hepatic toxicity are prominent with asparaginase use. The incidence of these side effects increases with age and makes asparaginase use more difficult in adult patients (13). He developed fever and was diagnosed with Pseudomonas pneumonia on day 10 of induction chemotherapy. Bone marrow aspiration on day 24 revealed 40% cellularity with no discernible blasts on morphological examination. Relapse is thought to be due to residual leukemia cells that are below the limits of detection using conventional morphological assessment. His peripheral smear revealed many large cells with reduced cytoplasm, fine chromatin, and poorly defined nucleoli. The patient achieved hematological and cytogenetic remission after cycle 1 of induction chemotherapy. Nelarabine has efficacy in the relapsed setting and has been evaluated in the frontline setting (26). However, larger studies are needed to establish the optimal schedule of nelarabine incorporation into frontline regimens as only 20% of the cohort received all intended courses of nelarabine. Which of the following is considered to be a good prognostic factor for above patient A 23-year-old man presents to the hospital with abdominal distention and skin rash. The liver is palpable 5 cm below the right costal margin and spleen is palpable 10 cm below the left costal margin. A complete blood cell count reveals a leukocyte count of 150,000/L, hemoglobin of 8. Following completion of induction and consolidation treatment, no minimal residual disease was detected by multiparameter flow cytometry. She has no sibling, and no human leukocyte antigen-matched donor is available in the bone marrow registry. Cord blood transplant Autologous stem cell transplant Continue dasatinib Start monthly vincristine, prednisone, 6-mercaptopurine, and methotrexate for 2 years (E) No further treatment needed 5. A 32-year-old man with Ph- B-acute lymphoblastic leukemia received induction and consolidation with a multiagent chemotherapy regimen. Which of the following enzyme deficiency best explains the need for dose reduction She commenced induction with a regimen containing vincristine, peg-asparaginase, daunorubicin and prednisone. Two weeks after starting induction, she was readmitted to the hospital with severe abdominal pain, nausea, and vomiting. Her physical examination revealed epigastric tenderness without any rebound, hypoactive bowel sounds. Which one of the following is the most likely etiology for above clinical presentation A 45-year-old woman with Ph+ acute lymphoblastic leukemia was treated with combination chemotherapy and imatinib. Subsequently, she underwent allogeneic stem cell transplant from a matched sibling donor. Immunophenotypes and karyotypes of leukemic cells in children with Down syndrome and acute lymphoblastic leukemia. Concurrent intensive chemotherapy and imatinib before and after stem cell transplantation in newly diagnosed Philadelphia chromosome-positive acute lymphoblastic leukemia. Alterations of chemotherapeutic pharmacokinetic profiles by drug-drug interactions. Prognostic importance of 6-mercaptopurine dose intensity in acute lymphoblastic leukemia. What determines the outcomes for adolescents and young adults with acute lymphoblastic leukemia treated on cooperative group protocols Adult patients with acute lymphoblastic leukemia and molecular failure display a poor prognosis and are candidates for stem cell transplantation and targeted therapies. Comparative analysis of flow cytometry and polymerase chain reaction for the detection of minimal residual disease in childhood acute lymphoblastic leukemia. The role of cytotoxic therapy with hematopoietic stem cell transplantation in the therapy of acute lymphoblastic leukemia in adults: an evidence-based review. Phase 1 multicenter study of vincristine sulfate liposomes injection and dexamethasone in adults with relapsed or refractory acute lymphoblastic leukemia. These changes limit normal differentiation and lead to proliferation of abnormal leukemic cells or blasts. Exposure to benzene, pesticides, petroleum products, and radiation increases the risk of developing leukemia. Erythroblasts are not counted as blasts except in the rare instance of pure erythroid leukemia. At a morphological level, this heterogeneity is manifested by variability in the degree of commitment and differentiation of the cell lineage. Immunophenotyping by flow cytometry is used to determine lineage involvement of a newly diagnosed acute leukemia. Flow cytometric determination of blast count should not be used as a substitute for morphological evaluation. Acute leukemias of ambiguous lineage are rare leukemias and comprise those cases that demonstrate no evidence of lineage differentiation. Conventional cytogenetic analysis is a mandatory component in the diagnostic evaluation of a patient with suspected acute leukemia. A minimum of 20 metaphase cells analyzed from bone marrow is considered mandatory to establish the diagnosis of a normal karyotype, and recommended to define an abnormal karyotype.