General Information about Estrace
Menopause is a natural and inevitable a part of a woman's life that occurs when she stops having her monthly interval. While this transition marks the top of a girl's reproductive years, it could additionally convey alongside a host of uncomfortable signs. The decrease in estrogen levels during menopause could cause hot flashes, vaginal dryness, burning, and irritation, making it a challenging time for so much of ladies. Fortunately, with the help of Estrace, these signs can be effectively managed.
Another common problem that girls expertise throughout menopause is vaginal dryness, which can result in discomfort and ache during intercourse. With the use of Estrace vaginal cream, women can discover aid from this symptom. The cream is inserted into the vagina and works by lubricating and moisturizing the vaginal tissues, making intercourse more snug and pleasant. It also helps to reduce burning and irritation within the vagina, a typical criticism during menopause.
In conclusion, menopause can be a difficult time for ladies because of the varied symptoms it brings. However, with the assistance of Estrace, these symptoms could be alleviated, providing ladies with much-needed reduction and permitting them to enjoy their day by day lives with out interruptions. As each lady's menopause journey is exclusive, it is essential to consult with a physician to find out the appropriate form and dosage of Estrace for their specific wants. With correct use and regular monitoring, Estrace might help ladies navigate by way of menopause more comfortably and with minimal disruption.
Estrace also helps to forestall a situation often recognized as vaginal atrophy, which is the thinning, drying, and inflammation of the vaginal walls as a result of lower in estrogen levels. This condition may cause discomfort and pain with intercourse and improve the danger of urinary tract infections. By utilizing Estrace, ladies can maintain the health of their vaginal tissues and stop these problems.
Estrace is a type of estrogen that is prescribed to deal with menopausal signs. It works by boosting the levels of estrogen in the body, which in turn helps to alleviate these bothersome symptoms. This medicine is on the market in numerous forms such as tablets, lotions, and vaginal rings, catering to the individual needs of girls.
It is worth noting that like all treatment, Estrace may have some side effects, corresponding to breast pain, bloating, and headaches. Women with a historical past of sure medical situations, similar to breast cancer, heart illness, or blood clots, should communicate to their doctor earlier than utilizing Estrace. Additionally, common check-ups are essential while taking this treatment to monitor its effectiveness and any potential unwanted facet effects.
Aside from managing menopausal symptoms, Estrace has also been discovered to produce other advantages for ladies. Studies have proven that it might possibly help to stop bone loss and scale back the danger of osteoporosis, a situation the place bones turn out to be weak and brittle. As estrogen performs a vital function in sustaining bone density, the utilization of Estrace may help to prevent bone loss and fractures in ladies going through menopause.
One of the most common signs of menopause is scorching flashes, that are sudden feelings of heat that may trigger intense sweating and reddening of the pores and skin. Estrace helps to scale back the frequency and intensity of hot flashes, allowing girls to go about their day with out being constantly disrupted by these uncomfortable sensations. By regulating estrogen levels, Estrace helps to stabilize physique temperature and reduce the incidence of hot flashes.
The salutary effects of antagonizing the angiotensin system in patients with Marfan syndrome appear to be explained in part by reductions in arterial stiffness womens health kettlebell estrace 1 mg buy low price. However, the findings from that study were mixed, and any signal toward clinical benefit in selected patients was offset by increased intracranial hemorrhage in the study population. Conclusions the pathobiology of vascular fibrosis is complex, which corresponds to the diversity of collagen biofunctionality observed across the spectrum of cardiovascular diseases. The synthesis and regulation of collagen fibrils is a highly coordinated biochemical event that may be stimulated by a wide range of insults commonly observed in cardiovascular diseases, such as necrosis, inflammation, thrombosis, hypoxia, and pathophysiological levels of profibrotic hormones. Cardiovascular fibrosis plays a crucial role in the pathology and clinical risk in many diseases; however, fibrosis-specific drug therapies generally remain lacking. Greater emphasis on the disease-specific mechanisms underlying fibrosis, rather than targeting master switch molecules alone, may provide much needed insight for the development of effective therapeutics to decrease or prevent fibrosis in affected patients. Upregulation of steroidogenic acute regulatory protein by hypoxia stimulates aldosterone synthesis in pulmonary artery endothelial cells to promote vascular fibrosis. Prognostic value of quantitative contrast-enhanced cardiovascular magnetic resonance for the evaluation of sudden death risk in patients with hypertrophic cardiomyopathy. Electrically unexcitable scar mapping based on pacing threshold for identification of the reentry circuit isthmus: feasibility for guiding ventricular tachycardia ablation. Trafficking mechanisms of extracellular matrix macromolecules: insights from vertebrate development and human disease. Mineralocorticoid receptor blockade reverses obesity-related changes in expression of adiponectin, peroxisome proliferator-activated receptor-gamma, and proinflammatory adipokines. Gly-X-Y tripeptide frequencies in collagen: a context for host-guest triple-helical peptides. Energies of peptide-peptide and peptide-water hydrogen bonds in collagen: evidences from infrared spectroscopy, quartzpiezo gravimetry, and differential scanning calorimetry. Evidence for a role of hydroxyproline in stabilizing the triple-helix of collagen. Mechanism of constitutive export from the Golgi: bulk flow via the formation, protrusion, and en bloc cleavage of large trans-Golgi network tubular domains. Common and unique mechanisms regulate fibrosis in various fibroproliferative diseases. Contribution of aldosterone to cardiovascular and renal inflammation and fibrosis. Aldosterone inactivates the endothelin-B receptor via a cysteinyl thiol redox switch to decrease pulmonary endothelial nitric oxide levels and modulation pulmonary arterial hypertension. Aldosterone impairs vascular reactivity by decreasing glucose-6-phosphate dehydrogenase activity. Regulation of cell invasion and morphogenesis in a three-dimensional type I collagen matrix by membrane-type matrix metalloproteinases 1, 2, and 3. Myocardial collagen cross-linking is associated with heart failure hospitalization in patients with hypertensive heart failure. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction. Association of fibrosis with mortality and sudden cardiac death in patients with nonischemic dilated cardiomyopathy. Occurrence and frequency of arrhythmias in hypertrophic cardiomyopathy in relation to delayed enhancement on cardiovascular magnetic resonance. Myocardial fibrosis on cardiac magnetic resonance and cardiac outcomes in hypertrophic cardiomyopathy: a meta-analysis. Fibrotic atrial cardiomyopathy, atrial fibrillation, and thromboembolism: mechanistic links and clinical inferences. Vascular fibrosis in aging and hypertension: molecular mechanisms and clinical implications. Selective mineralocorticoid receptor blocker eplerenone reduces resistance artery stiffness in hypertensive patients. Distinct effects of losartan and atenolol on vascular stiffness in Marfan syndrome. Transforming growth factor-1 represses bone morphogenetic protein-mediated Smad signaling in pulmonary artery smooth muscle cells via Smad3. Serum endostatin is a genetically determined predictor of survival in pulmonary arterial hypertension. Circulating collagen biomarkers as indicators of disease severity in pulmonary arterial hypertension. Monach Abstract "Vasculitis" encompasses many diseases that share the feature of inflammatory destruction of blood vessels but otherwise show fundamental differences. Diseases that affect large arteries appear to be mediated by T cell infiltration, starting with extravasation from the vasa vasorum, followed by local activation of macrophages and chronic inflammation. Diseases that affect venules, capillaries, and arterioles are mediated by neutrophils activated at the endothelium, leading to necrosis. Immune complex vasculitis is a generic mechanism downstream of many underlying causes. It is unclear whether vasculitides affecting small arteries always begin with a necrotizing, neutrophilic phase or can sometimes begin with a mononuclear infiltrate. In all the vasculitides, the outcome depends on the extent of vascular injury, the nature of the blood supply to the organs involved, and the capacity of those organs to heal. Keywords vasculitis; pathophysiology; aortitis; giant cell arteritis; polyarteritis nodosa; immune complex; antineutrophil cytoplasmic antibodies the term "vasculitis" encompasses diseases that share the feature of inflammatory destruction of blood vessels but otherwise include diverse clinical phenotypes and pathophysiologies. The rarity of the vasculitides and the paucity of animal models means that their pathophysiologies are not as well understood as in many other inflammatory diseases.
Larger pcdida breast cancer network of strength buy estrace master card, mch ~ those Including the infufor mesmteric vessels, will need to be damped, cut, and lig:aa:d separately. A surgeon then proceeds with additional procedures if necessary to complete the ovarian cancer dcbulking surgery. A colostomy or rectosigmoid anastomosis may require mobilization of the splenic flexure and is performed near the end of surgery. Urinary tract infection, pneumonia, deep-vein thrombosis, wound cellulitis, and postoperative ileus are relatively common events following major abdominal surgery fur ovarian cancer. Reoperation fur anastomotic breakdown or postoperative hemorrhage specific to en bloc pelvic resection is uncommon (Tozzi, 2017). Surgeries for Gynecologic Malignancies an omental cake are informed of a possible need for bowel resection, splencctomy, or other radical debulking procedures to remove the entire tumor. First, patients who present with advanced ovarian cancer almost invariably have metastases to the omentum. Thus, a surgeon is prepared to encompass the entire tumor with an adequate resection. Second, omentectomy is routindy indicated for staging patients with ovarian cancer or with uterine papillary serous carcinoma who do not have obvious metastatic disease (Armstrong, 2019; Whitney, 2010). Its anterior leaf attaches to the greater curvature of the stomach via the gastrocolic ligament. Inftacolic omentectomy describes transection of the anterior leaf (gastrocolic ligament) at a levd below the transverse colon. However, this surgery is typically performed with other gynecologic procedures that warrant antibiotics and YrE prophylaxis, as listed in Tables 39-8 and 39-10 (p. The decision to administer a bowel preparation regimen is individualized by surgeon preference and clinical setting. The posterior leaf of the omentum is best accessed by flipping the omental drape cephalad. Dissection generally begins as far to the right as possible and continues as far to the left as possible. Entrance into the lesser sac mobilizes the colon and provides access to the tumor-free proximal gastrocolic ligament. Omentectomy is typically performed as an inpatient procedure under general anesthesia. A patient is positioned supine, a Foley catheter is placed, and the abdomen is surgically prepared. However, because of the uncertain extent of disease that accompanies these cases, a midline vertical incision is most commonly sdected. If only a portion of the omentum needs to be removed for staging purposes, the incision docs not necessarily need to be extended above the umbilicus since the omentum is often accessible. In all other situations, the incision is extended cephalad to provide sufficient exposure. Consent Although bleeding may follow inadequate vessd ligation, complications from omentectomy are rare. Obesity results in a much thicker omentum that has thicker Vlllicuiar pedicles, which may slip from clamps or ligatures. Additionally, prior upper abdominal surgety-panicularly gastric bypass-may cause adhesions and a more difficult resection. This organ is directly beneath a midline vertical incision and should be readily visible. Omentectomy is typically the first procedure performed in women with an omental cake and presumed ovarian cancer. The omentum can usually be quickly removed and sent for fro:ren-section analysis while a surgeon places a self-retaining retractor and proceeds with the remainder of a planned operation. A surgeon gently grasps the infracolic omentum and pulls it out of the abdomen through the incision. The extent of resection can then be determined, and the abdominal wall incision extended if necessary. Next, attention turns to the anterior omental leaf, and the omencal drape is now flipped caudad. For an infracolic omentcctomy, dissection of the omentum is performed inferior to the level of the transverse colon. Numerous vertically coursing vessels can be seen, but others are covered by fatty tissue and difficult to appreciate. A right-angle clamp is used by the surgeon to "pop" through an avascular portion of the gastrocolic ligament that is near, but safely distal to , the colon. This procedure is continued across the entire gastrocolic ligament, and the omental specimen is handed off. However, if a J-Bap is planned instead of an omentectomy, then only three quarters of the omentum is divided from right to left. The distal tip of the flap is brought into the pdvis and tacked to adjoining peritoneum with 2-0 or 3-0 gauge ddayed-absorbable suture to provide additional blood supply wherever desired. Regardless of whether removing the infracolic omentum or fashioning a]-flap, the drape will need to be rotated back and forth intermittently to make certain that dissection remains away from the colon. In cases in which an omental cake has extended proximally, a supracolic (total) omentectomy is indicated.
Estrace Dosage and Price
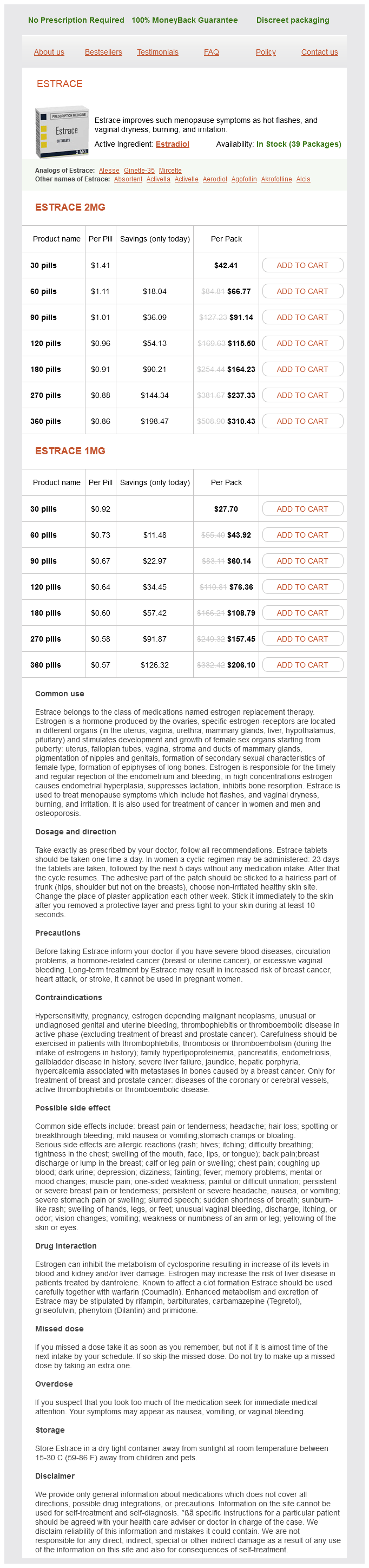
Estrace 2mg
- 30 pills - $42.41
- 60 pills - $66.77
- 90 pills - $91.14
- 120 pills - $115.50
- 180 pills - $164.23
- 270 pills - $237.33
- 360 pills - $310.43
Estrace 1mg
- 30 pills - $27.70
- 60 pills - $43.92
- 90 pills - $60.14
- 120 pills - $76.36
- 180 pills - $108.79
- 270 pills - $157.45
- 360 pills - $206.10
Moneta Abstract Mesenteric ischemia is a condition caused by compromised blood flow to the small and large intestines and may include gastric and hepatic circulations as well menstruation 7 days estrace 1 mg purchase online. Regardless of the cause of mesenteric ischemia, whether it be acute or chronic, one must have a high index of suspicion. Without consideration of mesenteric ischemia, the appropriate diagnostic evaluation is unlikely to be promptly obtained, resulting in needless additional morbidity and mortality. Keywords Acute mesenteric ischemia; chronic mesenteric ischemia; nonocclusive mesenteric ischemia; mesenteric venous thrombosis Clinical evaluation of possible mesenteric ischemia begins with an appropriate index of suspicion for the diagnosis followed by a careful history and physical examination. Although the various etiologies differ in their underlying pathologies and the clinical settings in which they occur, there may be significant overlap in their clinical presentation. The most crucial point is to understand the variety of clinical settings in which intestinal ischemia can occur and to include mesenteric ischemia in the differential diagnosis of patients presenting with abdominal pain. The goal is to achieve a rapid and efficient diagnosis prior to the onset of bowel infarction and resulting sepsis. Most patients with atherosclerotic mesenteric vascular disease are asymptomatic and at low risk for bowel infarction due to only mild to moderate stenosis of the mesenteric arteries and a robust collateral network that may compensate for reduced flow through one mesenteric artery. There are no signs of peritonitis, and the degree of pain may reflect the volume of the ingested meal. As the disease progresses, patients experience pain with each meal and may develop a fear of food, termed sitophobia. Duplex Ultrasonography Duplex ultrasonography can serve as a valuable noninvasive screening test for mesenteric artery stenosis and for follow-up in patients with mesenteric artery reconstructions. Duplex ultrasound can detect hemodynamically significant stenoses in splanchnic vessels. Some studies have used 50% luminal narrowing as a cutoff for significant stenosis, and others have delineated 70% luminal narrowing as significant stenosis in keeping with the Doppler criterion for significant stenosis. Limitations include contrast-related nephropathy, hypersensitivity reaction, and ionizing radiation exposure. Mesenteric Angiography Mesenteric angiography has traditionally been the gold standard for diagnosis of hemodynamically significant mesenteric artery stenosis. Operative repair, however, is associated with significant morbidity and mortality in most series. Endovascular treatment has high technical and early clinical success rates, with decreased morbidity and mortality compared to surgical intervention. Therefore, treatment decisions must be based on large case series in which a variety of procedures have been used. Indications for Operation Revascularization is indicated for symptomatic intestinal ischemia. The exposure is familiar, and risks of dissection and clamping are less than with more proximal aortic exposures. In addition, the procedure can be readily combined with other intraabdominal vascular procedures. The primary disadvantage is that the infrarenal aorta and iliac arteries are frequently calcified, increasing the technical difficulty of the proximal anastomosis. For these patients, vein grafts are preferred to minimize the possibility of graft infection. Special attention must be paid to graft configuration to avoid graft kinking when the graft is placed in a retrograde configuration. The graft is excluded from the peritoneal cavity by closing the mesenteric peritoneum, approximating the ligament of Treitz, and closing the posterior parietal peritoneum. After the inflow anastomosis is performed, the graft is arranged in an inverse "c" configuration. Antegrade bypass Antegrade bypasses originate from the anterior surface of the supraceliac aorta. Antegrade bypass provides prograde flow to the mesenteric vessels and is clearly the preferred approach in patients with contraindications to use of the infrarenal aorta or an iliac artery as a bypass origin. Visceral bypass grafts can be constructed with a partial-occlusion clamping of the aorta in many cases, although in most cases, the "partial" occlusion is actually near-total occlusion. Transient hepatic and renal ischemia is usually well tolerated, but is a potential disadvantage to the antegrade approach, particularly in patients with significant preexisting renal insufficiency. A disadvantage of the antegrade bypass is that the retropancreatic space is limited, and great care is necessary when tunneling the graft. Some surgeons advocate prepancreatic tunneling to avoid compression of the graft within the tunnel. A prepancreatic tunnel, however, places the graft in apposition to the posterior wall of the stomach and theoretically increases the possibility of graft infection. Multiple-Vessel Revascularization Versus Single-Vessel Revascularization One debated issue is the optimal number of vessels to revascularize. Proponents of multiple-vessel, or "complete" revascularization suggest that this approach makes recurrent symptomatic ischemia less likely should one graft or graft limb thrombose. More recent data also suggest that the rate of symptomatic recurrence, graft patency, and patient survival are unaffected by the number of revascularized vessels. A retrograde mesenteric bypass to the celiac and superior mesenteric arteries, with reimplantation of the inferior mesenteric artery performed from the proximal right common iliac artery. Postoperative Care Patients with chronic visceral ischemia often have significant ischemic bowel injury that requires time for recovery. Sitophobia may persist temporarily after revascularization and some are unable to achieve adequate oral nutrition following visceral revascularization for a prolonged period.