General Information about Fosamax
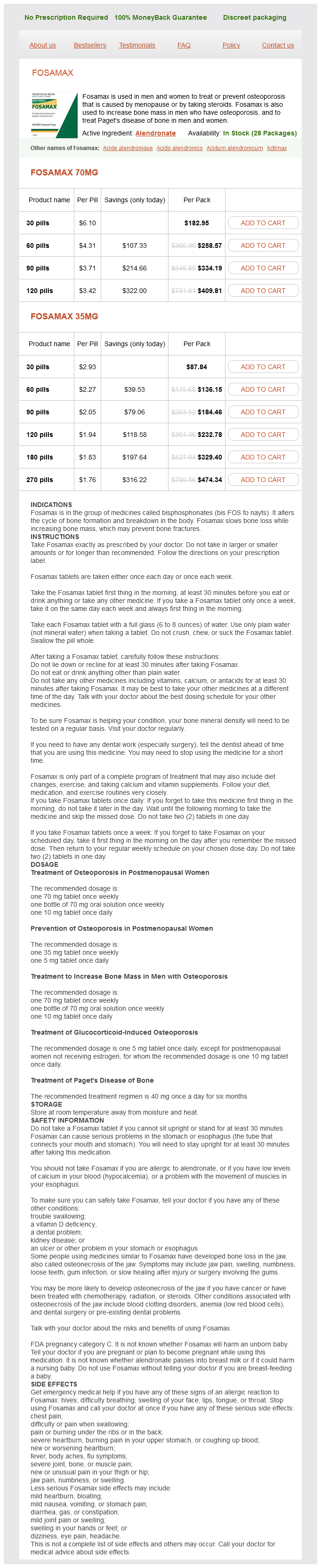
Fosamax, additionally identified by its generic name alendronate, is a prescription medicine that belongs to a class of medication called bisphosphonates. It is used to deal with and stop osteoporosis in both women and men. Fosamax works by slowing down the breakdown of bone and growing bone density, thus reducing the danger of fractures.
Moreover, Fosamax can be approved to be used in men who have osteoporosis. Although men are less prone to develop osteoporosis in comparison with ladies, they can still be affected. Fosamax has been confirmed to increase bone mass in men, making their bones stronger and less prone to fractures.
Like any treatment, Fosamax also has its share of unwanted side effects. Some widespread side effects of Fosamax include gentle gastrointestinal signs corresponding to nausea, indigestion, and diarrhea. In uncommon instances, it may find yourself in more extreme unwanted aspect effects, corresponding to jaw bone problems (osteonecrosis), esophageal ulcers, and irregular heartbeat. It is crucial to tell your doctor if you experience any of these symptoms whereas taking Fosamax.
Osteoporosis is a typical situation that affects millions of people, especially ladies after menopause. It is characterized by low bone density, making bones weaker and more vulnerable to fractures. In the United States alone, over 10 million folks have osteoporosis, and nearly 80% of them are ladies. To fight this situation, a number of medicines have been developed, and one such drug is Fosamax.
Fosamax can also be used to treat glucocorticoid-induced osteoporosis. Glucocorticoids, also called steroids, are used to deal with varied medical circumstances corresponding to asthma, rheumatoid arthritis, and lupus. However, prolonged use of these drugs can lead to bone loss. Fosamax helps improve bone density in people taking steroids, reducing their threat of osteoporosis.
Fosamax is obtainable in two forms – a pill and an oral answer. The tablet is normally taken once per week, while the oral solution is taken as quickly as a day. It is beneficial to take Fosamax on an empty stomach within the morning with a full glass of water. It is important to comply with the dosing instructions provided by your doctor fastidiously. This medicine must be taken persistently to get the best results.
Another situation that Fosamax is used to deal with is Paget's illness of bone. This is a persistent situation where there's abnormal bone development, resulting in weak bones which are extra vulnerable to fractures. Fosamax helps regulate the bone development, lowering the chance of fractures and bettering bone power.
One of the most typical causes of osteoporosis in women is menopause. During this stage, the physique produces less estrogen, a hormone that helps keep bone density. This lower in estrogen leads to bone loss, making postmenopausal girls extra vulnerable to osteoporosis. Fosamax has been proven to be efficient in stopping and treating osteoporosis in postmenopausal girls.
In conclusion, Fosamax is a extensively used medicine for treating and preventing osteoporosis in each men and women. Its capacity to increase bone density and scale back the risk of fractures has made it a popular choice amongst doctors and patients. However, it is important to comply with the dosing instructions fastidiously and inform your doctor of any unwanted facet effects or medical situations before beginning Fosamax. With proper use, Fosamax might help enhance bone well being and quality of life for those affected by osteoporosis.
Fosamax is not appropriate for everyone, and sure medical conditions can have an effect on its effectiveness. It is important to tell your physician in case you have any kidney illness, vitamin D deficiency, or are unable to sit or stand upright for no less than 30 minutes. Additionally, it is not beneficial for pregnant or breastfeeding ladies.
In the absence of Pax-6 expression pregnancy 4 weeks ultrasound purchase line fosamax, neither the nasal placodes nor the lens placodes form. The nasal placodes originate from the anterolateral edge of the neural plate before its closure. The two limbs of the mesenchymal elevations are the nasomedial and nasolateral processes. As a consequence, the frontonasal prominence, which depends on forebrain retinoids for supporting proliferation of its mesenchymal cells, is reduced. While the nasal primordia merge toward the midline during weeks 6 and 7, the nasomedial processes form the tip and crest of the nose along with part of the nasal septum, and the nasolateral processes form the wings (alae) of the nose. By 61/2 weeks, only a thin oronasal membrane separates the oral cavity from the nasal cavity. The epithelium on the nasal surface of the palate differentiates into a ciliated columnar type, whereas the epithelium takes on a stratified squamous form on the oral surface of the palate. With the fusion of the lateral palatal shelves, the nasal cavity is considerably lengthened and ultimately communicates with the upper pharynx. Similar to the other major sensory organs of the head, the epithelium of each nasal pit induces the surrounding neural crest mesenchyme to form a cartilaginous capsule around it. In a three-dimensionally complex manner, the medial parts of the nasal capsules combine with more centrally derived deep neural crest mesenchyme to form the midline nasal septum and ethmoid bones. During the third month, shelflike structures called nasal conchae form from the ethmoid bones on the lateral wall of the nasal cavity. These structures increase the surface area available for conditioning the air within the nasal cavity. Late in fetal life and for several years after birth, the paranasal sinuses form as outgrowths from the walls of the nasal cavities. A developing sinus is lined by respiratory mucosa and is able to grow out through the nasal capsule by means of local degeneration of the cartilage of the capsular wall. The size and shape of the paranasal sinuses have a significant effect on the form of the face during its postnatal growth period. At 6 to 7 weeks, a pair of epithelial ingrowths can be seen in each side of the nasal septum near the palate. In most mammals and many other vertebrates, the vomeronasal organs, which are lined with a modified olfactory epithelium, remain prominent and are involved in the olfaction of food in the mouth or sexual olfactory stimuli. Beginning in the embryonic period and continuing throughout life, the olfactory epithelium is able to form primitive sensory bipolar neurons, which send axonal projections toward the olfactory bulb of the brain. Preceding axonal ingrowth, some cells break free from this epithelium and migrate toward the brain. Some of these cells may synthesize a substrate for the ingrowth of the olfactory axons. Other cells migrating from the olfactory placode (specifically, the vomeronasal primordium) synthesize luteinizing hormonereleasing hormone and migrate to the hypothalamus, the site of synthesis and release of this hormone in adults. Physiological evidence shows that the olfactory epithelium is capable of some function in late fetal life, but full olfactory function is not attained until after birth. Historically, the germ layer of origin of the primordia of the salivary glands has been difficult to determine, but recent research suggests that they are derived from ectoderm. As with other glandular structures associated with the digestive tract, the development of salivary glands depends on a continuing series of epitheliomesenchymal interactions. The outgrowing glandular epithelium contains a primary duct region capped by an epithelial endbud. The parasympathetic nerves, in turn, produce vasoactive intestinal peptide, which promotes growth of the duct and formation of a lumen within it. Much of the development of an exocrine gland, such as the salivary glands, depends upon branching morphogenesis, which involves an interplay between the glandular epithelium and the extracellular matrix surrounding it. While the primary duct begins to mature, it forms a basement membrane around itself as a means of stabilizing the duct. Expansion is facilitated through enzymatic digestion of the basement membrane, which becomes perforated and more distensible. These will coalesce to form a continuous ductule, and the surrounding epithelial cells will constitute a branch of the overall duct system. Fibronectin and collagen fibers (wavy lines) are lined up lateral to the lobule and in the newly forming cleft. Numerous combinations and degrees of severity exist, ranging from a unilateral cleft lip to a bilateral cleft lip associated with a fully cleft palate. Structurally, cleft lip results from the lack of fusion of the maxillary and nasomedial processes. The premaxillary segment commonly protrudes past the normal facial contours when viewed from the side. The mechanism frequently underlying cleft lip is hypoplasia of the maxillary process. This prevents contact between the maxillary and nasomedial processes from being established. The extent of palatal clefting ranges from involvement of the entire length of the palate to something as minor as a bifid uvula. In other cases, cleft lip and cleft palate can be linked to the action of a Site of incisive foramen Primary palate 14 chemical teratogen. Experiments on mice have shown that the incidence of cleft palate after exposure to a dose of cortisone is strongly related to the genetic background of the mouse.
Identification of antihypertensive peptides from peptic digest of two microalgae women's health center queens blvd buy generic fosamax, Chlorella vulgaris and Spirulina platensis. Antihypertensive effects, molecular docking study, and isothermal titration calorimetry assay of angiotensin I-converting enzyme inhibitory peptides from Chlorella vulgaris. Effect of Chlorella on blood pressure, cerebral stroke lesions, hypertensive vascular change and life-span in spontaneously hypertensive rats. Purification and identification of angiotensin Iconverting enzyme inhibitors from the red alga Porphyra yezoensis. Separation and identification of angiotensin Iconverting enzyme inhibitory peptides from peptic digest of Hizikia fusiformis protein. Identification of an antihypertensive peptide from peptic digest of wakame (Undaria pinnatifida). Isolation of an antihypertensive peptide fome alcalase digest of Spirulina platensis. Spectrophotometric assay using o-phthaldialdehyde for determination of proteolysis in milk and isolated milk proteins. Spectrophotometric assay and properties of the angiotensin-converting enzyme of rabbit lung. Characterization of inhibition and stability of soy-protein-derived angiotensin I-converting enzyme inhibitory peptides. Angiotensin converting enzyme inhibitory activity of peptides isolated from Manchego cheese. Antihypertensive effects of hydrolysates of wakame (Undar pinnatifida) and their angiotensin-I-converting enzyme inhibitory activity. Antihypertensive effects of tryptic hydrolysate of casein on normotensive and hypertensive volunteers. Measuring angiotensin-I converting enzyme inhibitory activity by micro plate assays: Comparison using marine cryptides and tentative threshold determinations with captopril and losartan. Structure and activity of angiotensin I converting enzyme inhibitory peptides from sake and sake lees. Purification and identification of an angiotensin I-converting enzyme inhibitory peptide from cauliflower byproducts protein hydrolysate. Classification and antihypertensive activity of angiotensin I-converting enzyme inhibitory peptides derived from food proteins. Identification and quantification of inhibitors for angiotensin-converting enzyme in hypoallergenic infant milk formulas. Inhibition properties of dipeptides from salmon muscle hydrolysate on angiotensin I-converting enzyme. Structural requirements of angiotensin I-converting enzyme inhibitory peptides: Quantitative structure-activity relationship study of di- and tripeptides. Angiotensin I-converting enzyme inhibitory peptides derived from wakame (Undaria pinnatifida) and their antihypertensive effect in spontaneously hypertensive rats. Angiotensin-I-converting enzyme inhibitory peptides derived from food proteins and their physiological and pharmacological effects. Isolation of peptides with angiotensin I-converting enzyme inhibitory effect derived from hydrolysate of upstream chum salmon muscle. Here, both buckwheat and wheat albumin that inhibited mammalian -amylase in vitro suppressed blood glucose level elevation after starch loading in vivo, but it had no effect after glucose loading. In contrast to the non-competitive inhibition of wheat -amylase inhibitor, buckwheat albumin acted in a competitive manner. Although buckwheat -amylase inhibitor was readily hydrolysed by digestive enzymes, the hydrolysate retained inhibitory activity. Together with its thermal stability, this suggests its potential use in functional foods that prevent diabetes. These complications sometimes lead to blindness, renal failure, and food ulcer, which seriously affect health-related quality of life of patients. Ingestion of a substance that inhibits polysaccharide hydrolysis is an effective means to suppress the elevation of blood glucose levels [2]. Buckwheat flour has been used as an ingredient mainly for noodles and pancakes in Asian and European countries. Pepsin from porcine stomach mucosa and trypsin from bovine pancreas were obtained from Wako Pure Chemical Industries (Osaka, Japan). The supernatant was heated at 80 C for 20 min to denature non-heat-stable proteins and centrifuged at 15,000× g for 15 min at 4 C. The precipitate was dialysed against distilled water to re-solubilise the protein and centrifuged at 15,000× g for 15 min at 4 C. After lyophilisation of the supernatant, about 15 mg of protein dissolved in 20 mL of distilled water was applied to a Sephadex G-50 column (2. Fractions (5 mL) were collected and the -amylase inhibitory activity in each fraction was measured (see Section 2. The fractions showing more than 90% inhibitory activity against -amylase from porcine pancreas were collected and lyophilised. Measurement of -Amylase Inhibitor Activity the -amylase inhibitory activity was measured, as described by Foo and Bais, with some modifications [25]. The standard -amylase inhibition assay was carried out by preincubating 25 L of 1. The enzyme reaction was terminated by the addition of 100 L of 10% (v/v) Tris solution, after which the absorbance at 405 nm of the 2-chloro-4-nitrophenol that was produced by the reaction was measured. The inhibitory activity against -amylase from mealworms was measured by the same procedure except that the buffer used was 20 mM acetate buffer at pH 5.
Fosamax Dosage and Price
Fosamax 70mg
- 30 pills - $182.95
- 60 pills - $258.57
- 90 pills - $334.19
- 120 pills - $409.81
Fosamax 35mg
- 30 pills - $87.84
- 60 pills - $136.15
- 90 pills - $184.46
- 120 pills - $232.78
- 180 pills - $329.40
- 270 pills - $474.34
Early in their life history menstrual sponge cheap fosamax 35 mg mastercard, embryonic muscle fibers are innervated by motoneurons. Although it has long been assumed that fast and slow motoneurons impose their own functional characteristics on the developing muscle fibers, it now seems that they may select muscle fibers of a compatible type through information contained on their cell surfaces. Initially, a motor nerve may terminate on both fast and slow muscle fibers, but ultimately, inappropriate connections are broken, so fast nerve fibers innervate only fast muscle fibers, and slow nerves innervate only slow muscle fibers. The phenotypes of muscle fibers depend on the nature of the specific proteins that compose their contractile apparatus. There are qualitative differences in many of the contractile proteins between fast and slow muscle fibers, and within each type of muscle fiber is a succession of isoforms of major proteins during embryonic development. The myosin molecules possess adenosine triphosphatase activity, and differences in this activity account partly for differences in the speed of contraction between fast and slow muscle fibers. The myosin molecule undergoes a succession of isoform transitions during development. After injury to muscle in an adult, the regenerating muscle fibers undergo sets of cellular and molecular isoform transitions that closely recapitulate the transitions occurring in normal ontogenesis. These fibers respond to exercise by undergoing hypertrophy or becoming more resistant to fatigue. Many other types of cells can also modify their phenotypes in response to changes in the environment, but the molecular changes are not always as striking as those seen in muscle fibers. Gorlin Collection, Division of Oral and Maxillofacial Pathology, University of Minnesota Dental School, courtesy Dr. Quail/chick grafting experiments have clearly shown that the major groups of skeletal muscles in the trunk and limbs arise from myogenic precursors located in the somites. In the thorax and abdomen, the intrinsic muscles of the back (the epaxial muscles) are derived from cells arising in the dorsal myotomal lip, whereas ventrolateral muscles (hypaxial muscles) arise from epithelially organized ventral buds of the somites. Tendons of the epaxial muscles arise from the syndetome layer within the somites (see Box 6. In the limb regions, myogenic cells immigrate from the dorsal (extensor muscles) and ventral (flexor muscles) regions of the dermomyotome. These cells undergo an epitheliomesenchymal transformation through the action of c-met interacting with scatter factor, and while migrating they are prevented from differentiating through the influence of Pax-3. Cranial myogenic cells originating in similar regions of the occipital somites migrate into the developing tongue and diaphragm. At the lumbar levels, precursors of the abdominal muscles also move out of the epithelium of ventrolateral somitic buds. This process activates two early transcription factors (Six [sine oculis] and Eya [eyes absent]), which leads to a more intense expression of Pax3 and the expression of Lbx1, a homeobox gene that is exclusively expressed in the lateral dermomyotomal lips. The overall form of a muscle is determined principally by its connective tissue framework rather than the myoblasts themselves. Experiments have shown that myogenic cells from somites are essentially interchangeable. Myogenic cells from somites that would normally form muscles of the trunk can participate in the formation of normal leg muscles. More recent experiments have shown different cellular behavior in areas of the myotomes adjacent to limb and nonlimb regions. In thoracic segments, cells of the dermatome surround the lateral edges of the myotome; this is followed by an increase in the number of myotubes formed in the myotome and the penetration of the muscle primordia into the body wall. In contrast, at the levels of the limb buds, dermatome cells die before surrounding the early myotubes that form in the myotome. These myotubes neither increase significantly in number nor move out from the myotomes to form separate muscle primordia. Quail/chick grafting experiments have shown that the paraxial mesoderm, specifically the somitomeres, constitutes the main source of the cranial musculature. The cells that make up some of the extraocular muscles arise from the prechordal plate of the early embryo. Other craniofacial muscles, especially those in the lower jaw and neck, arise from lateral splanchnic mesoderm, as does cardiac muscle. In the early postgastrulation period, the lateral splanchnic mesoderm (sometimes called the cardiopharyngeal morphogenetic field), associated with the future pharynx and probably responding to the same inductive signals from the pharyngeal endoderm, gives rise to both the lower cranial musculature and the secondary heart field. Early in the determination process, both these types of muscle are under the control of transcription factors. As with muscles in the trunk, muscles in the head and neck arise by the movement of myogenic cells away from the paraxial mesoderm through mesenchyme (either neural crestderived or mesodermal mesenchyme) on their way to their final destination. Morphogenesis of muscles in the cranial region is determined by information inherent in the neural crestderived connective tissues that ensheathe the muscles. There is no early-level specificity in the paraxial myogenic cells; this has been determined by grafting somites or somitomeres from one craniocaudal level to another. Gata Contractile protein genes structures form muscles normal for the region into which they migrate, rather than muscles appropriate for the level of origin of the grafted somites. Certain muscles of the head, in particular muscles of the tongue, arise from the occipital somites in the manner of trunk muscles and undergo extensive migration into the enlarging head. Similar to the myogenic cells of the limb, precursor cells of the tongue musculature express Pax-3 while they are migrating into the head. Despite their final location in the head, these muscles are subjected to the same types of early molecular regulation of myogenesis (Myf-5, Myf-6) as trunk muscles. Cardiac Muscle Although a striated muscle, cardiac muscle differs from skeletal muscles in many aspects of embryonic development. Differences between the differentiation of cardiac and skeletal muscle appear early because MyoD and other common master regulators of skeletal muscle differentiation are not expressed in early cardiac muscle development. Early cardiac and skeletal muscle cells express isoforms of molecules that are characteristic of mature cells of the other type.