General Information about Lotrisone
Another benefit of Lotrisone is that it's comparatively safe to use. Side results such as itching, burning, or stinging at the website of software are uncommon, and extreme allergic reactions are very rare. However, as with any medication, it is important to observe the directions rigorously and solely use Lotrisone as directed by a doctor or pharmacist.
Fungal infections can happen virtually wherever on the body, from the scalp, feet, and nails, to the groin, hands, and even the inside of the mouth. They could be caused by quite a lot of fungi, including dermatophytes, yeasts, and molds. These infections can typically be difficult to treat, and if left untreated, can result in severe problems. Thankfully, Lotrisone is right here to help.
In addition to its effectiveness in treating fungal pores and skin infections, Lotrisone can be known for its ease of use. It could be applied on to the affected space, and only must be used a couple of times a day, relying on the severity of the an infection. Lotrisone also comes in convenient, moveable packaging, making it simple to take with you wherever you go.
Lotrisone has been confirmed to be extremely effective in treating a wide range of fungal skin infections, similar to athlete's foot, jock itch, ringworm, and yeast infections. It works by attacking the root reason for the infection, offering quick relief from signs and stopping the infection from spreading. This not only helps to alleviate discomfort but also speeds up the therapeutic course of and reduces the chance of complications.
In conclusion, Lotrisone is a safe, effective, and convenient treatment for fungal skin infections. Its mixture of betamethasone and clotrimazole makes it a strong weapon in opposition to a selection of fungi, offering quick relief from signs and selling therapeutic. However, it is necessary to observe that Lotrisone is not beneficial for use in kids underneath the age of 17, or pregnant or lactating women, except specifically instructed by a doctor. If you're experiencing signs of a fungal pores and skin an infection, consult your doctor or pharmacist to see if Lotrisone is the right remedy for you.
Lotrisone is a well-liked antifungal medicine that has been broadly used for treating skin infections caused by varied kinds of fungi. The lively ingredients in Lotrisone, betamethasone and clotrimazole, work together to inhibit the growth of fungi, providing relief from signs and serving to to clear up the infection. This highly effective mixture makes Lotrisone extremely effective in treating a variety of fungal skin infections, and it is suggested by doctors and pharmacists alike.
One of the best issues about Lotrisone is that it's out there in numerous varieties, including cream and lotion, making it suitable for a wide selection of skin types and conditions. Lotrisone cream is often used to treat infections that occur between the toes, while the lotion is more suited for treating infections on larger skin surfaces. This versatility makes it a preferred selection amongst each sufferers and healthcare professionals.
The two active elements in Lotrisone, betamethasone and clotrimazole, work in numerous methods to deal with fungal infections. Betamethasone is a sort of corticosteroid that helps to scale back irritation and alleviate signs such as redness, swelling, and itching. Clotrimazole, then again, is an antifungal agent that works by inhibiting the growth of fungi, stopping them from reproducing and spreading. Together, these two ingredients work to supply fast-acting relief and get rid of the source of the infection.
These mutations are observed in approximately 60% of melanomas fungus under toe lotrisone 10 mg for sale, as well as 40% of thyroid cancers, and 20% of colon cancer and ovarian cancer. Temsirolimus at a weekly dose of 25 mg administered intravenously is licensed for treatment of previously untreated, metastatic renal cell carcinoma based on phase 3 trial results showing improved survival for patients receiving temsirolimus compared with that for patients receiving interferon alfa. Objective responses to rapamycin have been observed in tuberous sclerosis patients with subependymal giant cell astrocytomas, providing evidence for sufficient rapamycin brain penetration for clinical effect. However, there is evidence from studies of immature mice for a continued role for the Hedgehog pathway postnatally, as short-term treatment with pathway inhibitors leads to permanent bone damage. Pediatric evaluations of this class of agents will require careful monitoring for skeletal growth complications, given the bone effects observed for Hedgehog pathway inhibitors in immature mice. The concept of combining an agent that depletes the cancer stem cell population with conventional therapy that induces tumor debulking is an attractive, though unproven, application of Hedgehog pathway inhibitors. Targeting Notch Pathway Signaling Notch pathway signaling is implicated in a wide range of developmental and cellular processes, including carcinogenesis. Each of these classes of inhibitors has a strong preclinical package, with potent in vitro activity and convincing in vivo activity against a range of xenografts. Given the specificity of these agents for actively dividing cells, they share a similar clinical toxicity profile in which neutropenia and/or thrombocytopenia are common dose-limiting toxicities. Histone acetylation alters chromatin structure and induces a local chromatin environment conducive with gene transcription, whereas histone deacetylation is commonly associated with repression of transcription. Additional substrates include nuclear proteins such as p53, myo-D, and E2F1 and cytoplasmic proteins such as a-tubulin and Hsp90. Polyubiquitinated proteins are recognized by the proteasome and degraded into small polypeptides. A subsequent phase 3 trial demonstrated that bortezomib was significantly more effective than dexamethasone for patients with relapsed multiple myeloma who had received one to three previous therapies. Targeting Angiogenesis From 1971 when Folkman proposed targeting angiogenesis as a potential effective strategy for cancer treatment,503 three decades were required to prove that antiangiogenic therapy could improve survival for patients with cancer. Glioblastoma is a tumor characterized by vascular proliferation and high expression of angiogenic factors, and bevacizumab induces objective responses, either as a single agent or in combination with irinotecan, in adults with glioblastoma. The first study addressing this question was for colorectal cancer, and randomized patients to standard chemotherapy for 6 months with or without 12 months of bevacizumab. The failure of bevacizumab in the adjuvant setting to aid in controlling micrometastatic disease, if confirmed in other studies, has major implications for the use of this class of agents in the pediatric oncology setting, given the primary focus on curative therapy for children with cancer. In vivo testing primarily showed tumor growth delay, with very few examples of tumor regression observed. When treatment was stopped, tumors quickly resumed growth, consistent with results from adult cancer models indicating that continuous treatment is necessary for tumor growth inhibition. Another approach to blocking angiogenesis is to target the interactions between V3 and V5 integrin adhesion molecules on sprouting capillary cells and their extracellular matrix ligands. New targets for antiangiogenic therapy include components of the Notch pathway such as Dll4 and the angiopoietins (Ang-1 and Ang-2) and their receptor (Tie2). For decades, there have been consistent improvements in outcome as a result of clinical trials that intensified and refined therapy with standard cytotoxic agents. Advances using this strategy have slowed down for most childhood cancers, and others have stopped altogether. One of the opportunities is the large number of targeted agents in clinical trials that block growth and survival signaling pathways used by cancer cells. This opportunity is the converse of one of the key challenges to successfully employing targeted agents to improve outcome: the selection of truly effective agents to study against specific patient populations from among the scores of agents potentially available for study. There is cause for optimism in addressing this challenge, given the availability of technologies that should allow delineation within the coming decade of all of the recurring genomic and epigenomic alterations present in most childhood cancers. Understanding the genomic alterations that define each childhood cancer will provide invaluable information for prioritizing agents for investigation. Also encouraging is the availability of increasingly sophisticated technologies for target identification and validation, and the presence of molecularly characterized in vivo models for developing reliable preclinical assessments of the antitumor activity of novel agents. Another important challenge is the increasing need to study subsets of patients with a particular cancer diagnosis based on the molecular characteristics of their cancer. Meeting this challenge will require pediatric clinical trials infrastructures becoming more proficient in evaluating new therapies in genomically defined subtypes of childhood cancers. Given the relatively limited numbers of children with any given cancer diagnosis and the even smaller number within any given diagnosis that have a specific molecular abnormality, meeting this challenge will increasingly involve international collaborations so that sufficient patient numbers can be enrolled onto clinical trials to define the contribution of novel agents for patient populations whose cancers have specific molecular characteristics. If pediatric oncology researchers can take advantage of the available opportunities related to molecularly targeted agents, then there is cause for optimism that meaningful progress will be made in the coming decade toward having curative therapy available for every child diagnosed with cancer. Validation of a therapeutic target identified by gene expression based classification. Emerging drugs for the therapy of primary and post essential thrombocythemia, post polycythemia vera myelofibrosis. Phosphorylation profiles of protein kinases in alveolar and embryonal rhabdomyosarcoma. Methodological approaches in application of synthetic lethality screening towards anticancer therapy. Kinase mutations and imatinib response in patients with metastatic gastrointestinal stromal tumor. Genomic alterations of anaplastic lymphoma kinase may sensitize tumors to anaplastic lymphoma kinase inhibitors. In: Proceedings of the 100th Annual Meeting of the American Association for Cancer Research. Suppression of the Shh pathway using a small molecule inhibitor eliminates medulloblastoma in Ptc1(+/-p53(-/-) mice.
A case of malignant rhabdoid tumor arising from soft parts in the prepubic region fungus gnats mmj order genuine lotrisone line. Malignant soft tissue neoplasms with the histologic features of renal rhabdoid tumors: an ultrastructural and immunohistochemical study. The existence of rhabdoid cells in specified soft tissue sarcomas: histopathological, ultrastructural and immunohistochemical evidence. Molecular analysis of a partial deletion of 22q in a central nervous system rhabdoid tumor. Malignant rhabdoid tumor: a highly malignant childhood tumor with minimal karyotypic changes. Cytogenetic characteristics of a malignant rhabdoid tumor arising from the paravertebral region. Localization of Beckwith-Wiedemann and rhabdoid tumor chromosome rearrangements to a defined interval in chromosome band 11p15. Molecular sublocalization and characterization of the 11;22 translocation breakpoint in a malignant rhabdoid tumor. A new advance in alternative splicing databases: from catalogue to detailed analysis of regulation of expression and function of human alternative splicing variants. Transcriptional landscape of the human and fly genomes: nonlinear and multifunctional modular model of transcriptomes. Exploring the metabolic and genetic control of gene expression on a genomic scale. Sensitivity and specificity of five abundance estimators for high-density oligonucleotide microarrays. Searching for evidence of altered gene expression: a comment on statistical analysis of microarray data [editorial; comment]. Diagnostic and prognostic prediction using gene expression profiles in high-dimensional microarray data. Classification of multiple cancer types by multicategory support vector machines using gene expression data. Gene expression profiling identifies clinically relevant subtypes of prostate cancer. Diffuse large B-cell lymphoma outcome prediction by gene-expression profiling and supervised machine learning. Gene expression profiles that segregate patients with childhood acute lymphoblastic leukaemia: an independent validation study identifies that endoglin associates with patient outcome. Evaluation of a linear amplification method for small samples used on high-density oligonucleotide microarray analysis. Evaluation of procedures for amplification of small-size samples for hybridization on microarrays. Patterns of single-nucleotide polymorphisms in candidate genes for blood-pressure homeostasis. Chromosome-wide distribution of haplotype blocks and the role of recombination hot spots. Linkage disequilibrium mapping via cladistic analysis of single-nucleotide polymorphism haplotypes. Applying a new generation of genetic maps to understand human inflammatory disease. Strong association of the Y402H variant in complement factor H at 1q32 with susceptibility to age-related macular degeneration. Novel genomic imbalances in embryonal rhabdomyosarcoma revealed by comparative genomic hybridization and fluorescence in situ hybridization: an Intergroup Rhabdomyosarcoma Study. Diverse immunoreactivity and metachronous ultrastructural variability in fatal primitive childhood tumor with rhabdoid features [letter]. Identification of a plasma proteomic signature to distinguish pediatric osteosarcoma from benign osteochondroma. Proteomic analysis of the stroma-related proteins in nasopharyngeal carcinoma and normal nasopharyngeal epithelial tissues [published online ahead of print February 26, 2009]. Morphogenomics and morphoproteomics: a role for anatomic pathology in personalized medicine. Convergence of biomarkers, bioinformatics and nanotechnology for individualized cancer treatment. Malignant ectomesenchymoma of soft tissue: report of two cases and review of the literature. Pediatric aggressive fibromatosis: a retrospective analysis of 13 patients and review of literature. Superficial low-grade fibromyxoid sarcoma (Evans tumor): a clinicopathologic analysis of 19 cases with a unique observation in the pediatric population. Low-grade fibromyxoid sarcoma and hyalinizing spindle cell tumor with giant rosettes: a clinicopathologic study of 73 cases supporting their identity and assessing the impact of high-grade areas. Expression of anaplastic lymphoma kinase in soft tissue tumors: an immunohistochemical and molecular study of 249 cases. Gene expression analysis of soft tissue sarcomas: characterization and reclassification of malignant fibrous histiocytoma. Angiomatoid "malignant" fibrous histiocytoma: a clinicopathologic study of 158 cases and further exploration of the myoid phenotype. Angiomatoid (malignant) fibrous histiocytoma: a peculiar low-grade tumor showing immunophenotypic heterogeneity and ultrastructural variations. Sublocalization of the synovial sarcoma-associated t(X;18) chromosomal breakpoint in Xp11. Plexiform malignant peripheral nerve sheath tumor of infancy and childhood [see comments].
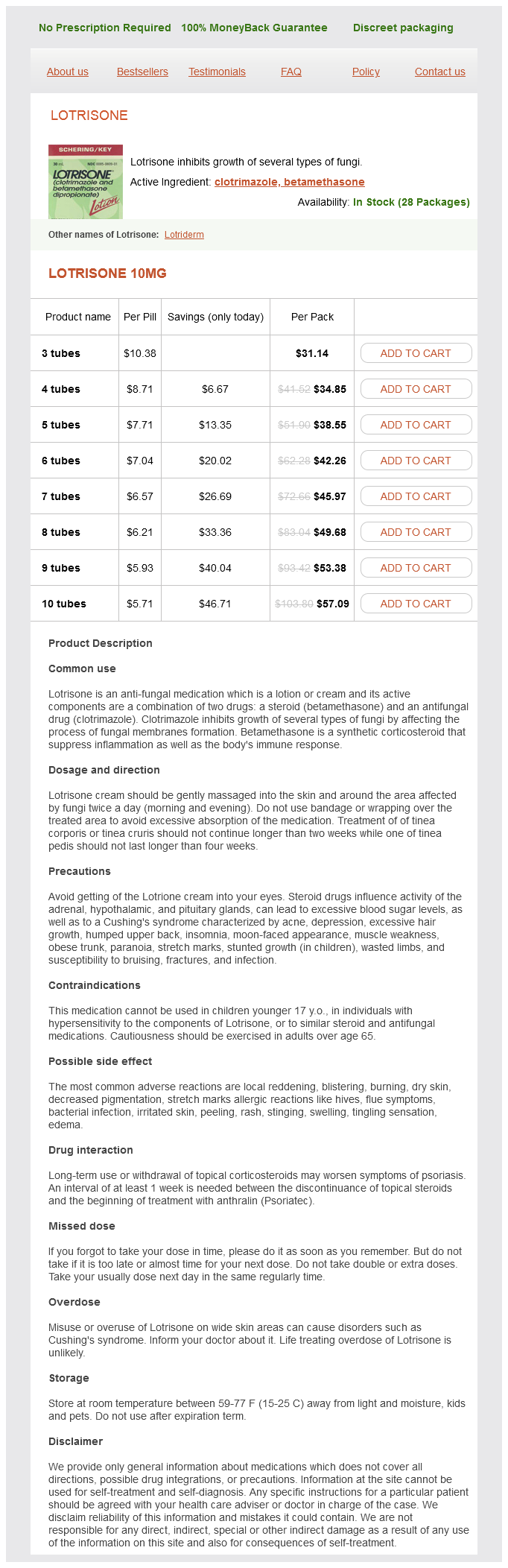
Lotrisone Dosage and Price
Lotrisone 10mg
- 3 tubes - $31.14
- 4 tubes - $34.85
- 5 tubes - $38.55
- 6 tubes - $42.26
- 7 tubes - $45.97
- 8 tubes - $49.68
- 9 tubes - $53.38
- 10 tubes - $57.09
Initial radiation injury at the macromolecular and cellular levels results in release of inflammatory cytokines fungus gnats fox farm purchase 10 mg lotrisone with mastercard, growth factors, and further reactive oxygen species, with resultant hypoxia, chronic oxidative stress, and fixed tissue damage. The timing of the acute pneumonitis phase is within the 1- to 4-month post-irradiation subacute interval. Later, progressive pulmonary fibrosis can be apparent within 6 to 12 months or several years after therapy, marked by accumulation of fibrin and atypical fibroblasts thickening the alveolar interstitial tissues. Heart Cardiac effects following irradiation in children and adolescents are most commonly seen in Hodgkin lymphoma, where there are considerable data re incidence and apparent pathophysiology. It is uncommon to see evolution toward significant pericardial fibrosis or chronic, constrictive changes. The pathophysiology is classically related to capillary endothelial damage with consequent luminal obstruction, fibrin formation, and platelet thrombi leading to ischemia, myocardial cell death, and fibrosis. In adults, renal tolerance is typically quoted at 20 to 25 Gy fractionated dose to more than 50% of the functioning renal volume. Renal tolerance defines treatment planning for tumors in this region, requiring limitation of dose to at least 50% of the renal volume to levels typically below 14 to 16 Gy in children whose treatment includes irradiation and chemotherapy, with particular attention to cisplatin. In its more severe clinical presentation, signs mimic the hemolytic-uremic syndrome. Earlier reports of frequent radiation-related enteropathy, often requiring surgical management for small bowel obstructive disease, have largely been resolved with more experience in coordinating surgery, abdominal and/or pelvic irradiation, and chemotherapy. Reactions tend to be greater after pre-irradiation surgery (with adhesions often "fixing" bowel into the low abdomen-pelvis). Symptoms often mimic small bowel inflammatory disease, although there is a noted lack of C-reactive protein elevation in radiation-related late bowel injury. Jude protocol for local irradiation) showed diminished hormonal secretion in two-thirds of cases, including almost half the children/adolescents with localized posterior fossa tumors. Acute changes are uncommon; radiation "edema" or worsening of tumoralterations in ovarian endocrine secretions are noted following doses as low as 250 to 400 cGy. In low-grade tumors, the phenomenon is typically confined and self-limited; in high-grade gliomas or brain stem gliomas, subacute changes mimic the "pseudoprogression" noted in adult malignant gliomas. In areas outside the primary tumor, but typically within the high-dose radiation region, one can see parenchymal areas of focal white matter reactivity or apparent leptomeningeal changes mimicking tumor involvement as a subacute phenomenon; such signs usually abate spontaneously over several months but can progress to frank necrosis. Focal necrosis is typically seen only with doses in excess of 60 Gy; the incidence is greatly increased with dose per fraction in excess of 240 to 300 cGy. The small, convoluted collateral vessels adjacent to the occluded major vessels produce a pattern on angiography termed puff of smoke or moyamoya in Japanese. Postirradiation vascular changes can also manifest as cavernomas, most of which are benign, if occasionally associated with intracranial hemorrhage. Although classically accepted as showing myelopathy at dose levels of 50 Gy or more, recent data have been interpreted to show a 5% risk of myelopathy at 59 Gy, with only a 0. Noting concerns regarding cisplatin administration and irradiation as ototoxic interventions, P. Cisplatin-related ototoxicity is early, bilateral, and dose-related, appearing as high-frequency sensorineural loss during a course of cisplatin chemotherapy. Radiation-related ototoxicity is a late, random event occurring as an acute, unilateral, irreversible hearing loss. Radiation ototoxicity occurs beyond 35 years post-therapy following doses of more than 35 to 50 Gy to the cochlea (absent cisplatin). B: Imaging 3 months after completion of radiation therapy, at which point, long tract signs increased significantly, requiring corticosteroid management. The patient has no residual long tract signs and is essentially normal on neurologic examination. Treatment of the whole brain or areas most associated with learning and memory (hippocampus, medial P. In most pediatric settings, there is a dose response relationship within the therapeutic dose range of 15 to 60 Gy. Large cohorts of pediatric Hodgkin lymphoma survivors have recently been analyzed to confirm the incidence of secondary solid tumors, largely related to radiation therapy, exceeding 7% to 10% at 20 years and 25% at 30 years posttherapy-a relative incidence of 14 to 18 times that of the normal, age-adjusted population. Also to be noted is the occurrence of benign neoplasms-thyroid adenomas, osteochondromas, and breast fibroadenomas. Jude combining irradiation with high-dose antimetabolite therapy ultimately showed an incidence of secondary malignant gliomas of 12% to 20%. A gene expression model of intrinsic tumor radiosensitivity: prediction of response and prognosis after chemoradiation. Molecular predictors of progression-free and overall survival in patients with newly diagnosed glioblastoma: a prospective translational study of the German Glioma Network. The histological structure of some human lung cancers and the possible implications for radiotherapy. The phenomenon of reoxygenation and its implications for fractionated radiotherapy. Oxygen distribution in squamous cell carcinoma metastases and its relationship to outcome of radiation therapy. Carbogen breathing with nicotinamide improves the oxygen status of tumours in patients. Modification of hypoxia-induced radioresistance in tumors by the use of oxygen and sensitizers. External beam radiation of tumors alters phenotype of tumor cells to render them susceptible to vaccine-mediated T-cell killing. Changes in early and late radiation responses with altered dose fractionation: implications for dose-survival relationships. Potential reduction of the incidence of radiation-induced second cancers by using proton beams in the treatment of pediatric tumors. Development of fast neutron therapy worldwide: radiobiological, clinical and technical aspects.