General Information about Metoclopramide
While way of life modifications and over-the-counter medicines can successfully handle GERD symptoms in many individuals, some individuals could require prescription treatment to alleviate their discomfort. This is where metoclopramide is out there in. It works by stimulating the muscular tissues in the digestive tract, which helps to move food from the stomach into the intestines, lowering the probability of stomach acid refluxing again into the esophagus. In addition to treating GERD, metoclopramide is also used to treat diabetic gastroparesis, a condition in which the stomach takes longer than normal to empty its contents.
Metoclopramide, a medication also identified as Reglan, is a widely used drug for the management of gastroesophageal reflux illness (GERD) in patients who have not responded to other treatment options. It belongs to the category of medication known as prokinetic brokers, which are used to improve the movement of meals by way of the digestive tract. Metoclopramide has been approved by the united states Food and Drug Administration (FDA) for short-term therapy of GERD signs, and its effectiveness and security have been well-established by way of years of clinical use.
One of the principle benefits of metoclopramide is its fast-acting nature. It starts to work inside 30 minutes and might present aid for as a lot as 2 hours, making it an appropriate option for sufferers experiencing acute GERD symptoms. This fast onset of motion could be particularly helpful for patients who expertise frequent symptoms or for individuals who have not had success with other therapy choices.
While metoclopramide is considered a secure and efficient medicine for the treatment of GERD, it isn't with out potential unwanted effects. The most typical unwanted aspect effects reported with its use include drowsiness, fatigue, and restlessness. More critical however rare unwanted aspect effects can also occur, similar to involuntary muscle actions, seizures, and extreme allergic reactions. Therefore, it's crucial for sufferers to debate their medical historical past and any present drugs they're taking with their doctor earlier than beginning metoclopramide to make sure its secure use.
Additionally, metoclopramide should only be used for short-term treatment of GERD, usually no longer than 12 weeks. Long-term use of this medication has been associated with a severe situation called tardive dyskinesia, which involves involuntary, repetitive movements of the face and physique. Therefore, it is necessary for sufferers to comply with their physician's directions carefully and not to exceed the beneficial duration of therapy.
In conclusion, metoclopramide is a well-known and relied upon treatment for the treatment of GERD symptoms in sufferers who haven't responded to other therapies. It is safe and efficient when used in the short-term and might present much-needed aid for individuals fighting this continual situation. As all the time, sufferers should talk about their remedy choices with their healthcare provider to find out if metoclopramide is the best selection for them.
GERD, also called acid reflux, is a persistent condition that happens when abdomen acid and contents circulate again into the esophagus, inflicting uncomfortable symptoms similar to heartburn, chest ache, and difficulty swallowing. It is a common dysfunction that affects roughly 20% of the inhabitants within the United States and might have a significant impact on a person's high quality of life. GERD may be attributable to a variety of components, such as a weak decrease esophageal sphincter (the muscle that closes off the stomach from the esophagus), weight problems, or a hiatal hernia.
While you work chronic gastritis rheumatoid arthritis purchase metoclopramide 10 mg on line, check the questions in the laboratory Review Sheet section for this exercise. A number of the questions there refer to some of the observations you are asked to make during your microscopic study. Epithelium Lamina propria Function: Wraps and cushions organs; its phagocytes engulf bacteria; plays important role in inflammation; holds and conveys tissue fluid. The connective tissues perform a variety of functions, but they primarily protect, support, and bind together other tissues of the body. For example, bones are composed of connective tissue (bone or osseous tissue), and they protect and support other body tissues and organs. Ligaments and tendons (dense regular connective tissue) bind the bones together or bind skeletal muscles to bones. Connective tissue also serves a vital function in the repair of all body tissues: many wounds are repaired by connective tissue in the form of scar tissue. Connective tissues are composed of many types of cells, and there is a great deal of nonliving material between the cells. The nonliving material between the cells-the extracellular matrix-distinguishes connective tissue from all other tissues. The matrix, secreted by the cells, is primarily responsible for the strength associated with connective tissue, but its firmness and relative amount vary. Depending on its makeup, the ground substance may be liquid, gel-like, or very hard. When the matrix is firm, as in cartilage and bone, the connective tissue cells reside in cavities in the matrix called lacunae. The fibers, which provide support, include collagenic (white) fibers, elastic (yellow) fibers, and reticular (fine collagenic) fibers. Photomicrograph: Areolar connective tissue from the lamina propria of a mucous membrane (340:). Classification of Tissues 43 (b) Adipose tissue Description: Matrix as in areolar, but very sparse; closely packed adipocytes, or fat cells, have nucleus pushed to the side by large fat droplet. Function: Fibers form a soft internal skeleton (stroma) that supports other cell types. Photomicrograph: Adipose tissue from the subcutaneous layer under the skin (350:). Photomicrograph: Dark-staining network of reticular connective tissue fibers forming the internal skeleton of the spleen (350:). Shoulder joint Location: Forms most of the embryonic skeleton; covers the ends of long bones in joint cavities; forms costal cartilages of the ribs; cartilages of the nose, trachea, and larynx. Ligament Costal cartilages Tendon Function: Attaches muscles to bones or to muscles; attaches bones to bones; withstands great tensile stress when pulling force is applied in one direction. Function: Supports and reinforces; has cushioning properties; resists compression. Classification of Tissues 45 (f) Fibrocartilage Description: Matrix similar but less firm than in hyaline cartilage; thick collagen fibers predominate. Location: Bones 5 Intervertebral discs Function: Tensile strength with the ability to absorb compressive shock. Function: Bone supports and protects (by enclosing); provides levers for the muscles to act on; stores calcium and other minerals and fat; marrow inside bones is the site for blood cell formation (hematopoiesis). For example, notice that the matrix of the dense fibrous connective tissue of tendons is packed with collagenic fibers and that the fibers are all running in the same direction. Activity 3 Examining Muscle Tissue Under the Microscope Go to station 3 of the demonstration area to examine prepared slides of skeletal, cardiac, and smooth muscle. Neuroglia are special supporting cells that protect, support, and insulate the more delicate neurons. The neurons are highly specialized to receive stimuli and to conduct impulses to all parts of the body. They are the cells that are most often associated with nervous system functioning. Neurons all have a nucleus-containing cell body, and their cytoplasm is drawn out into long extensions (cell processes)-sometimes as long as 3 feet (about 1 m), a characteristic that allows a single neuron to conduct an impulse over relatively long distances. Muscle tissue is specialized to contract (shorten) to produce movement of some body parts. As you might expect, muscle cells are elongated to provide a long axis for contraction. Skeletal muscle cells are long, cylindrical, and multinucleate (several nuclei per cell); they have obvious striations (stripes). As it contracts, the heart acts as a pump, propelling the blood into the blood vessels. Like skeletal muscle, it has striations, but cardiac cells are branching cells with one nucleus (or occasionally two) that fit together at junctions called intercalated discs that allow cardiac muscle to act as a unit. Cardiac muscle is under involuntary control, which means that we cannot voluntarily or consciously control the operation of the heart. Smooth muscle is found mainly in the walls of all hollow organs (digestive and urinary tract organs, uterus, blood vessels) except the heart. Typically two layers run at right angles to each other, so the muscle can constrict or dilate the lumen (cavity) of an organ and also propel substances along existing pathways.
Azathioprine chronic gastritis zinc discount metoclopramide 10 mg on line, gold (intramuscular or oral), hydroxychloroquine and penicillamine are used less frequently. Prognosis Prognosis is variable: some patients will have minimal disability after many years and others will be severely disabled, with most patients between these extremes. A poor prognosis is indicated by the following: insidious onset, female sex, increasing number of joints involved, level of disability at onset, higher inflammatory and autoimmune markers and signs of early erosive damage on imaging. Axial spondylarthritis this is an inflammatory disorder of the spine, affecting mainly young adults. Other features include Achilles tendinitis and plantar fasciitis (enthesitis) and tenderness around the pelvis and chest wall. In the spinal column, blurring of the upper or lower vertebral rims at the thoracolumbar junction is caused by an enthesitis at the insertion of the intervertebral ligaments. In advanced disease there is calcification of the interspinous ligaments and fusion of the facet joints as well as syndesmophytes at all levels. Management Early diagnosis and treatment is essential to prevent irreversible syndesmophyte formation and progressive calcification. With effective treatment, most patients are able to lead a normal active life and remain at work. Psoriatic arthritis Arthritis occurs in 10% of patients with psoriasis, particularly in those with nail disease (p. Reactive arthritis Reactive arthritis is a sterile synovitis, which occurs following: Gastrointestinal infection with Shigella, Salmonella, Yersinia or Campylobacter Sexually acquired infection non-specific urethritis in the male or cervicitis in the female due to infection with Chlamydia trachomatis or Ureaplasma urealyticum. Persistent bacterial antigen in the inflamed synovium of affected joints is thought to drive the inflammatory process. Clinical features the typical case is a young man who presents with an acute arthritis shortly (within 4 weeks) after an enteric or sexually acquired infection, which may have been mild or asymptomatic. The joints of the lower limbs are particularly affected in an asymmetrical pattern; the knees, ankles and feet are the most common sites. Circinate balanitis causes superficial ulcers around the penile meatus, which harden to a crust in the circumcised male. Red plaques and pustules that resemble pustular psoriasis (keratoderma blenorrhagica) are found on the palms and soles of the feet. It usually parallels the activity of the inflammatory bowel disease and consequently improves as bowel symptoms improve. Gout and hyperuricaemia Gout is an inflammatory arthritis caused by hyperuricaemia and intra-articular sodium urate crystals. The disease is five times more common in men, occurs rarely before young adulthood (when it suggests a specific enzyme defect), and seldom occurs in pre-menopausal females. Pathogenesis Hyperuricaemia results from overproduction of uric acid or renal underexcretion (Table 7. Idiopathic (primary) gout is the most common form and most patients have impaired renal excretion of uric acid. Clinical features Hyperuricaemia and deposition of sodium urate crystals result in four clinical syndromes: Acute sodium urate synovitis acute gout Chronic interval gout Chronic polyarticular gout Chronic tophaceous gout Urate renal stone formation (p. Acute gout presents typically in a middle-aged male with sudden onset of severe pain, swelling and redness of the metatarsophalangeal joint of the big toe. The signs of inflammation may extend beyond the joint, giving the impression of cellulitis. The attack may be precipitated by dietary or alcoholic excess, by dehydration or by starting a diuretic. Acute attacks must be differentiated from other causes of monoarthritis, particularly septic arthritis. Presentation can also be with a polyarticular inflammatory arthritis, particularly in elderly women on long-term diuretics. Chronic tophaceous gout presents with large, smooth, white deposits (tophi) in the skin and around the joints, particularly on the ear, the fingers and on the Achilles tendon. However, the diagnosis is excluded if the serum uric acid is in the lower half of the normal range. It has a narrow therapeutic window and is extremely toxic in overdose (diarrhoea, abdominal pain, multi-organ failure). Obese patients should lose weight, alcohol consumption should be reduced and drugs such as thiazides and salicylates should be withdrawn. A diet which reduces total calorie and cholesterol intake and avoids purine-rich foods (offal, some fish and shellfish and spinach) is advised. Patients with frequent attacks (more than two per year) despite dietary changes or with gouty tophi or renal impairment are treated with allopurinol. Allopurinol inhibits xanthine oxidase (an enzyme in the purine breakdown pathway) and reduces serum urate levels rapidly. Febuxostat is a non-purine analogue inhibitor of xanthine oxidase that is well tolerated and as effective as allopurinol. Their costeffectiveness in managing gout resistant to conventional agents is still subject to trials. Asymptomatic hyperuricaemia is not usually treated unless plasma levels are very high or in patients with cancer to prevent the tumour lysis syndrome (p. Pseudogout (pyrophosphate arthropathy) Deposition of calcium pyrophosphate dihydrate in articular cartilage and periarticular tissue produces the radiological appearance of chondrocalcinosis (linear calcification parallel to the articular surfaces).
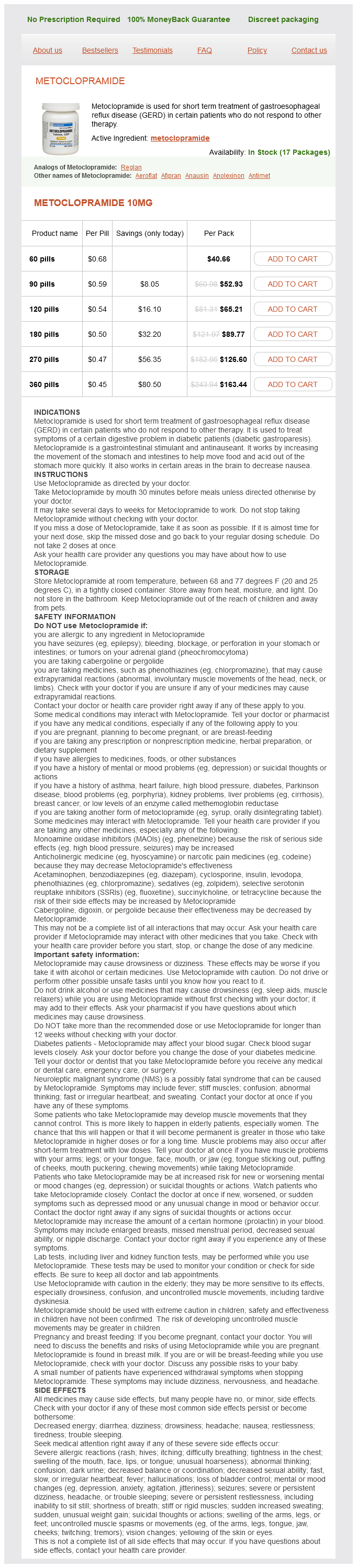
Metoclopramide Dosage and Price
Metoclopramide 10mg
- 60 pills - $40.66
- 90 pills - $52.93
- 120 pills - $65.21
- 180 pills - $89.77
- 270 pills - $126.60
- 360 pills - $163.44
A dural sinus gastritis in spanish buy metoclopramide 10 mg low price, the superior sagittal sinus, is enclosed by the dural membranes superiorly. Arachnoid villi, which return cerebrospinal fluid to the dural sinus, are also shown. Skull Superior sagittal sinus Scalp Dura mater Transverse sinus Arachnoid mater over medulla oblongata (a) Temporal bone Skin of scalp Periosteum Bone of skull Periosteal Meningeal Dura mater Superior sagittal sinus Subdural space Subarachnoid space Arachnoid mater Pia mater Arachnoid villus Blood vessel Falx cerebri (in longitudinal fissure only) 14 (b) secures the brain in the cranial cavity. The cavity created at this point is the large superior sagittal sinus, which collects blood draining from the brain tissue. The middle layer, the weblike arachnoid mater, underlies the dura mater and is partially separated from it by the subdural space. Its threadlike projections bridge the subarachnoid space and attach to the innermost membrane, the pia mater. Specialized projections of the arachnoid tissue called arachnoid villi protrude through the dura mater to allow the cerebrospinal fluid to drain back into the venous blood via the superior sagittal sinus and other dural sinuses. The cerebrospinal fluid is continually formed by the choroid plexuses, small capillary knots hanging from the roof of the ventricles of the brain. Cerebrospinal fluid forms a watery cushion that protects the delicate brain tissue against blows to the head. Activity 3 Tracing the Pathway of Cerebrospinal Fluid in the Brain Obtain a threedimensional model of the ventricles, and trace the path of cerebrospinal fluid circulation through the internal brain cavities from the lateral ventricles to the subarachnoid space. Testing methods Person is asked to sniff and identify aromatic substances, such as oil of cloves and vanilla. Vision and visual field are determined with eye chart and by testing the point at which the person first sees an object (finger) moving into the visual field. Eye interior viewed with ophthalmoscope to detect swelling of optic disc (point at which optic nerve leaves the eye) and to observe blood vessels. Pupillary reflex is tested with penlight (pupils should constrict when illuminated). Sensations of pain, touch, and temperature are tested with safety pin and hot and cold objects. Motor branch assessed by asking person to clench the teeth, open the mouth against resistance, and move the jaw side to side. Anterior two-thirds of tongue is tested for ability to taste sweet (sugar), salty, sour (vinegar), and bitter (quinine) substances. Oculomotor Mixed-motor fibers to inferior oblique and superior, inferior, and medial rectus muscles, which direct eyeball; to levator palpebrae muscles of eyelid; to iris and smooth muscle controlling lens shape and pupil size. Mixed-provides motor fibers to superior oblique muscle (an extrinsic eye muscle). Mixed-conducts sensory impulses from skin of face and anterior scalp, from mucosae of mouth and nose. Mixed-supplies motor fibers to muscles of facial expression and to lacrimal and salivary glands; carries sensory fibers from taste receptors of anterior tongue. Glossopharyngeal Purely sensory-transmits impulses for senses of equilibrum and hearing. Mixed-motor fibers serve pharyngeal muscles and salivary glands; sensory fibers carry impulses from pharynx, posterior tongue (taste buds), and pressure receptors of carotid artery. Mixed-motor fibers serve muscles of tongue and sensory fibers carry impulses from tongue. Sternocleidomastoid and trapezius muscles are checked for strength by asking person to rotate head and elevate shoulders against resistance. The cranial nerves are part of the peripheral nervous system, but they are best identified during the study of the brain. Only one pair, the vagus nerves, extends into the thoracic and abdominal cavities. The cranial nerves are numbered in order, and in most cases their names reflect the major structures they control. A catchy saying that might help you to remember the cranial nerves in order is "On occasion our trusty truck acts funny-very good vehicle anyhow. Most cranial nerves are mixed nerves (containing both motor and sensory fibers), but three pairs-optic, olfactory, and vestibulocochlear-are purely sensory. Those of the mixed cranial nerves are found both in the brain and in peripheral ganglia. Notice that the first (olfactory) cranial nerves are not visible on the model because they consist only of short axons that run from the nasal mucosa through the cribriform plate of the ethmoid bone. However, the synapse points of the first cranial nerves, the olfactory bulbs, are visible on the model, so identify these. Relatively speaking, which of these structures is obviously much larger in humans Place the ventral surface of the sheep brain down on the dissecting tray and observe the fragments of the dura mater. Gently force the cerebral hemispheres apart lat erally to expose the corpus callosum, the huge fiber tract deep to the longitudinal fissure. Notice that like the human brain, its surface is thrown into convolu tions (fissures and gyri). Identify the arachnoid mater, which appears on the brain surface as a delicate "cottony" material spanning the fissures. Look for the clublike olfactory bulbs on the inferior surface of the frontal lobes of the cerebral hemispheres. Moving posteriorly from the midbrain, identify first the pons and then the medulla oblongata.