General Information about Phenergan
Phenergan, additionally identified by its generic name promethazine, is a drugs that is used to deal with varied kinds of allergy signs. It belongs to a category of drugs known as antihistamines, which work by blocking the results of histamine within the physique. Histamine is a chemical that is released by the body in response to allergens, such as pollen, mud, or pet dander. By blocking histamine, Phenergan helps to alleviate symptoms such as itching, runny nostril, sneezing, itchy or watery eyes, hives, and itchy skin rashes.
Phenergan's sedative results ought to be used with warning, as they will trigger drowsiness and impair alertness. It is essential to observe the dosage directions rigorously and avoid working heavy equipment or driving while beneath the affect of Phenergan.
Phenergan should not be utilized in youngsters under the age of two, as it might increase the chance of respiratory despair. It must also be used with warning in the aged or those with respiratory or liver circumstances, as they might be more sensitive to its side effects.
Phenergan is available in numerous types, including tablets, suppositories, and syrup. It could be taken orally or rectally, and is usually prescribed as needed for symptom reduction. The dosage and frequency of use might range relying on the individual's age, medical situation, and response to the medicine.
One of the benefits of Phenergan is that it is efficient in treating varied forms of allergy symptoms. It is usually used for respiratory allergy symptoms, such as hay fever or allergic rhinitis, which is characterised by runny nostril, sneezing, and itchy nose and throat. Phenergan also can provide aid for skin allergy symptoms, corresponding to hives and itchy rashes, as properly as eye allergy symptoms, such as itchy, watery, or red eyes.
In uncommon circumstances, some individuals may have an allergic response to Phenergan. Symptoms of an allergic response could include hives, problem respiratory, and swelling of the face, lips, tongue, or throat. If any of those symptoms occur, instant medical consideration should be sought.
While Phenergan is mostly secure and well-tolerated, it can trigger some side effects similar to dry mouth, dizziness, blurred vision, and constipation. These side effects are often gentle and will diminish over time, but you will want to discuss any considerations with a healthcare provider.
In addition to its antihistamine properties, Phenergan has sedative effects that may help with symptoms similar to stressed sleep or nervousness due to allergies. This can be especially helpful for people who expertise difficulty in falling or staying asleep because of their allergic reactions.
In conclusion, Phenergan is a commonly prescribed medication for the therapy of various allergy symptoms. Its effectiveness in relieving symptoms such as itching, runny nostril, and hives, along with its sedative properties, make it a preferred selection for people seeking aid from allergies. However, it is very important use it as directed and be conscious of potential unwanted facet effects. Consult a healthcare supplier for customized advice on its usage and dosage.
If hydronephrosis is caused by an acute obstructive uropathy (any disease of the urinary tract) anxiety symptoms nervous stomach cheap phenergan 25 mg without a prescription, the patient may develop a paralytic ileus. In addition to renal failure, other complications include fluid and electrolyte imbalances, urinary stasis, renal calculus formation, hypertension, infection, sepsis, and septic shock. The most common types of obstruction are caused by prostate hypertrophy (enlargement), renal calculi that form in the renal pelvis or drop into the ureter, or urethral strictures. More unusual causes include structure of the ureter or bladder outlet, tumors pressing on the ureter, congenital abnormalities, pregnancy, cancer, blood clots, and a neurogenic bladder. There is evidence supporting possible contributions at several different loci resulting in genetic heterogeneity for this condition. Men 60 and older with prostate difficulties have a higher risk of hydronephrosis than women of the same age. The most common causes of hydronephrosis in women are gynecological cancers and pregnancy; because of the frequency of these conditions, rates of hydronephrosis are higher in women than men. In young adults, calculi are the most common 532 Hydronephrosis causes of hydronephrosis, whereas in children, reflux and ureteropelvic junction obstruction are the most common causes. Determine if the patient has a history of any chronic conditions such as diabetes mellitus, genitourinary or gynecological cancer, or prostate problems. Elicit a careful history about urinary patterns to determine a history of burning sensations or abnormal color. The patient may be completely anuric (no urine flow) or experience polyuria (large urine output) or nocturia (excessive urination at night) because of a partial urinary obstruction. Determine any recent history of mild or severe renal or flank pain that radiates to the groin or a history of fever. Establish any history of blood clots, bladder problems, or prior urinary difficulties. The most common symptoms are pain and changes in urinary pattern (anuria, polyuria, or nocturia). Upper ureteral or renal pelvic obstruction may lead to flank pain, whereas lower ureteral obstruction may cause pain radiating to the labia or scrotum. Inspect the flank area for asymmetry, which indicates the presence of a renal mass. Inspect the male urethra for stenosis, injury, or phimosis (narrowing so that the foreskin cannot be pushed back over the glans penis). When the flank area is palpated, a large fluctuating soft mass may be felt in the kidney area that represents the collection of urine in the renal pelvis. If the hydronephrosis is the result of bladder obstruction, markedly distended urinary bladder may be felt. Gentle pressure on the urinary bladder may result in leaking urine from the urethra because of bladder overflow. Rectal examination may reveal enlargement of the prostate or renal or pelvic masses. Although hydronephrosis is a treatable condition, the patient is likely to be upset and anxious. Urinary catheterization can also be a stressful event, particularly if it is performed by someone of the opposite gender. Diagnostic Highlights Test Ultrasonography Serum creatinine Normal Result Normal kidney and ureters 0. When no infection is present, immediate surgery is not necessary even if there is complete obstruction and anuria. Urologists often place a ureteral stent, which is performed along with a cystoscopy and retrograde pyelography. Stents can bypass an obstruction and dilate the ureter for further evaluation and treatment such as a percutaneous nephrostomy tube, which may be placed when a retrograde stent cannot be passed because of an obstruction in the ureter. Advances in endoscopic and percutaneous instrumentation have reduced the surgical role, although some cases of hydronephrosis still require treatment with open surgery. Many surgeons will wait until acid-base, fluid, and electrolyte balances are restored before operating. Surgery includes options such as prostatectomy for benign prostatic hypertrophy, tumor removal, and dilation of urethral strictures. When bilateral complete urinary obstruction is relieved, the patient usually has massive polyuria and excessive natriuresis (sodium loss in the urine). In general, the physician will prescribe the replacement of two-thirds of the loss of urinary volume per day to be replaced by salt-containing intravenous solutions. With impaired renal function, a diet low in sodium, potassium, and protein is often 534 Hydronephrosis prescribed. Preoperative diet restrictions are sometimes used to limit the progression of renal failure before surgical removal of the obstruction. Inspect the tube insertion site for signs of infection (purulent drainage, swelling, redness) and bleeding. If the tube is obstructed, follow the appropriate protocol for either irrigation or physician notification. Pharmacologic Highlights Medication or Drug Class Antibiotics Dosage Varies with drug Description Anti-infectives to manage bacterial infections: Trimethoprim sulfamethoxazole (Bactrim, Septra), ciprofloxacin hydrochloride (Cipro) Acetaminophen; mild narcotics Rationale Treatment based on bacterial sensitivity as well as the ability of the antibiotic to concentrate in the urinary system; course of treatment is at least 14 wk Relieve pain Analgesics Varies with drug Independent the patient requires careful fluid balance. Weigh the patient at the same time of day on the same scale with the same clothing.
Auscultation reveals high-pitched inspiratory and expiratory wheezes anxiety 6 letters 25 mg phenergan purchase, but with a major airway obstruction, breath sounds may be diminished. As the obstruction improves, breath sounds may actually worsen as they can be auscultated throughout the lung fields. During the most severe attacks of asthma, wheezing may be absent because of severe reduction of airflow, or its absence. A rapid heart rate, mild systolic hypertension, and a paradoxic pulse may also be present. Airway obstruction is generally managed with quick relief medications such as short-acting bronchodilators, systemic corticosteroids, and ipratropium (Atrovent). Unless contraindicated by a cardiac problem, 3,000 to 4,000 mL/day of fluid is usually administered intravenously, which helps loosen secretions and facilitates expectoration of the secretions. For the patient with increasing airway obstruction, endotracheal intubation and perhaps mechanical ventilation may be needed to maintain adequate airway and breathing. Close follow-up is needed when patients are discharged from the hospital because airway hyperactivity usually persists for 4 to 6 weeks after the event. To prevent symptoms, long-term control medications such as inhaled corticosteroids, inhaled cromolyn, long-acting bronchodilators, theophylline, leukotriene modifiers, and anti-IgE antibodies are used. Cromolyn sodium decreases bronchospasm, but it is not effective for acute bronchospasms and is used as a preventive measure. Independent Maintenance of airway, breathing, and circulation is the primary consideration during an acute attack. Patients should be on bedrest to minimize their oxygen consumption and to decrease the work of breathing. Note that patients usually assume a position to ease breathing; some patients breathe more easily while sitting in an upright position: Do not impose bedrest on a patient who can breathe only in another position. Ask questions that can be answered by nodding or a brief one-word answer so the patient can conserve energy for breathing. If the patient is a child, allow the parents to stay with the child during acute attacks. Have the parents identify a security item that reassures the child, such as a special blanket or toy, and keep the item with the child at all times. Reinforce coping strategies to the parents, and allow them to express any feelings of guilt and helplessness. For strategies to prevent future attacks, discuss triggers that can induce asthma attacks and ways to avoid them. If the attack is triggered by an allergen, explore with the patient or family the source and discuss possible strategies for eliminating it. Instruct the patient to notify the physician should she or he develop a respiratory infection that could trigger an attack. Explain to patients on steroid inhalers the need to rinse their mouths out after using them to avoid getting thrush. The authors used a qualitative analysis of transcripts from 33 recorded primary care visits. When providers did not have this knowledge about their patients, two themes arose: asthma self-management and healthy lifestyles. The authors concluded that when providers understood patient beliefs, they could initiate conversations that were meaningful to their asthma patients about their self-management. To prevent asthma attacks, teach patients the triggers that can precipitate an attack. In rare instances, asthma can lead to respiratory failure if patients are not treated immediately or are unresponsive to treatment (status asthmaticus). Explain that any dyspnea unrelieved by medications and accompanied by wheezing and accessory muscle use needs prompt attention from a healthcare provider. Encourage patients to identify and avoid things that make their asthma worse and to keep track of their symptoms. Teach the patient and family the correct use of medications, including the dosage, route, action, and side effects. When the airway becomes completely obstructed, the gas distal to the obstruction becomes 140 Atelectasis absorbed into the pulmonary circulation and the lung collapses. When gas is removed from portions of the lungs, unoxygenated blood passes unchanged through capillaries (a process called shunting), and hypoxemia results. The obstruction, which occurs at the level of the larger or smaller bronchus, can be caused by a foreign body, a tumor, or mucous plugging. When the obstruction is removed, the lungs return to normal unless infection persists. Nonobstructive atelectasis is caused by loss of contact between the parietal and the visceral pleurae, as well as compression, loss of surfactant, and replacement of parenchymal tissue by scarring or infiltrative disease. Pleural effusions, pneumothorax, blunt trauma, and acute respiratory distress syndrome all are nonobstructive conditions. Abnormal breathing patterns, such as hypoventilation following surgical procedures, can also lead to atelectasis. In such cases, the lung does not fully expand, which causes the lower airways to collapse. Patients with abdominal and/or thoracic surgery are the most susceptible, especially in the older age group. Patients in surgery for more than 4 hours have a 50% incidence of severe atelectasis, compared with a 19% incidence for those in surgery for 2 hours.
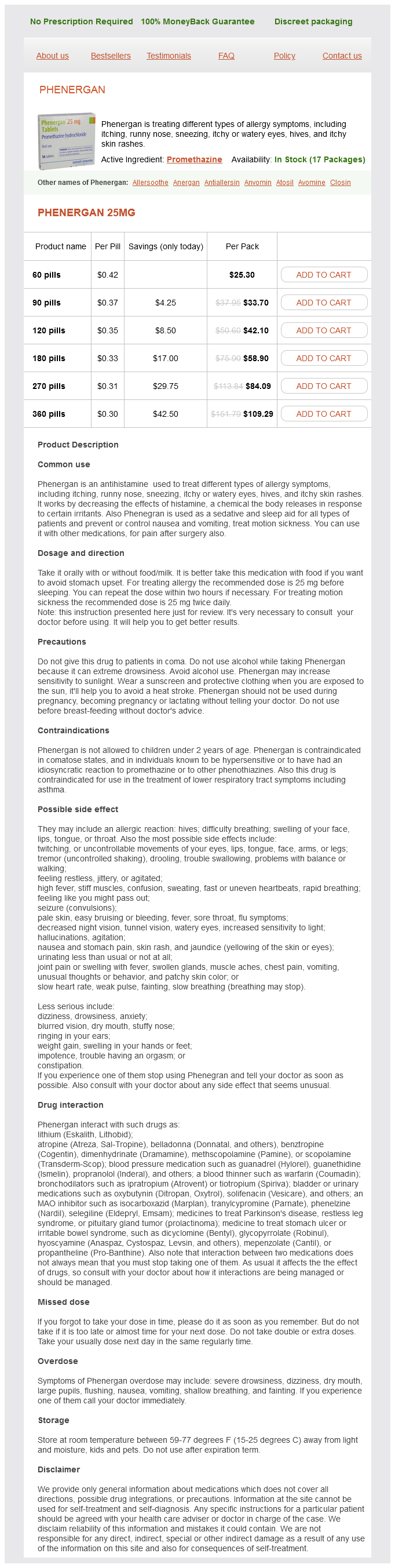
Phenergan Dosage and Price
Phenergan 25mg
- 60 pills - $25.30
- 90 pills - $33.70
- 120 pills - $42.10
- 180 pills - $58.90
- 270 pills - $84.09
- 360 pills - $109.29
Determine if the symptoms are milder in the morning anxiety 2 days before menses buy phenergan in india, worsen as the day progresses, and subside after short rest periods. Ask the patient if the head bobs when she or he is tired or if the jaw hangs open. You may note a masklike or "snarling" appearance because of the involvement of the facial muscles. Note if the patient has weak neck muscles that cause difficulty in maintaining head position that increases as the day progresses. Perform an eye examination Myasthenia Gravis 797 to determine visual acuity and eye movement, which are often abnormal. Myasthenic crisis is caused by undermedication and is also characterized by hypoxia (associated with tachycardia and possible elevated blood pressure), absence of the cough and gag reflexes, ptosis, diplopia and mydriasis (large pupils), and a positive response to the medication edrophonium (Tensilon). In comparison, a cholinergic crisis results from excessive anticholinesterase medication and is likely to occur within 45 to 60 minutes after the last drug dose. Side effects of overmedication include diarrhea and abdominal cramping, bradycardia and possible hypotension, a flushed diaphoretic appearance, miosis (small pupils), and increased secretions (saliva, tears, and bronchial secretions). Response to Tensilon is negative, and twitching and "thick tongue" dysphagia may occur. Depression may occur in patients who experience exacerbations and functional limitations in their lifestyles and role responsibilities. Plasmapheresis is reserved for patients who are refractory to conventional therapy, during myasthenic or cholinergic crisis, for prethymectomy stabilization and possible reduction in postthymectomy ventilator therapy, or if unacceptable drug side effects develop. Thymectomy increases the chance of remission, increases long-term survival, decreases the chance of relapse after stopping immunosuppressant therapy, and allows better control of the disease. Improvement is recognized in 60% to 70% of thymectomy patients and coincides with complete remission in 20% to 40% of cases (although this remission may require several years to occur). In addition to the drugs in the following table, immunoglobulins and monoclonal antibodies may be used. Instruct the patient to swallow only when the chin is tipped downward and never to speak with food in his or her mouth. To prevent pulmonary complications, encourage the patient to perform deep breathing and coughing to enhance ventilation. If the patient requires surgery, instruct him or her on chest splinting during deep-breathing and coughing exercises. Ensure adequate nutritional intake and observe for signs and symptoms of dehydration or malnutrition. Work with the patient and family to plan for foods that are easy to chew and swallow but are still appealing to the patient. Fear of sudden respiratory distress and the inability to call for help or to reach a call light is very real. Emphasize clear, honest communication about the realistic expectations of therapy because the time between initiation of the intervention and when the patient experiences improvement can be quite prolonged. Because treatment and improvement revolve around receiving the optimal dosages of medication, teach patients to recognize their disease status and the indications for self-determined dosage alterations to achieve an optimally effective drug benefit. Also teach the patients how to recognize the early signs of an overdose in order to prevent cholinergic crisis and when to self-medicate with atropine for relief of side effects. Because these patients are frequently responsible for determining drug alterations at home, denying their judgment in determining drug dosages can cause them to feel very vulnerable and insecure. Delays in receiving their medications can cause distrust and may result in significant physical difficulty in swallowing the delayed medication. Social disadvantage associated with myasthenia gravis and its treatment: A multicentre cross-sectional study. Factors promoting social disadvantage were severity of illness, dose of corticosteroids, and depression about change in appearance from corticosteroids. Be alert to factors that can cause exacerbations, such as infection (an annual flu shot is suggested), surgery, pregnancy, exposure to extreme temperatures, and tonic and alcoholic drinks. Instruct the patient and family about drug actions and side effects, the indications for dosage alteration, and the selective use of atropine for any overdose. It is advisable to time the dose 1 hour before meals for best chewing and swallowing. Explain the potential drug interactions (especially aminoglycosides and neuromuscular blocking agents, which include many pesticides). Encourage the patient to inform the dentist, ophthalmologist, and pharmacist of the myasthenic condition. Suggest that they collect a packet of literature to take to the emergency department in case the available physician is unfamiliar with this disease. Suggest having an "emergency code" to alert family if they are too weak to speak (such as ringing the phone twice and hanging up). Instruct the family about cardiopulmonary resuscitation techniques, how to perform the Heimlich maneuver, how to contact the rescue squad, and how to explain the route to the hospital. Make a referral to a vocational rehabilitation center if guidance for modifying the home or work environment, such as a raised seat and handrail for the toilet, would be beneficial. In addition, more than 50% of sudden deaths occur within 1 hour of the onset of symptoms. When myocardial tissue is deprived of oxygenated blood supply for a period of time, an area of myocardial necrosis develops; this necrosis is surrounded by injured and ischemic tissue.