General Information about Revectina
Parasites are organisms that stay and feed off their hosts, typically inflicting hurt and discomfort. These organisms can infect varied elements of the body, together with the intestines, skin, and even the eyes. Some of the most common parasitic infections embody roundworms, pinworms, whipworms, and scabies.
While Stromectol could also be efficient in treating parasitic infections, it's not a substitute for proper hygiene and sanitation practices. Washing your arms frequently, particularly before meals, and avoiding contact with contaminated water and meals might help prevent parasitic infections. It can additionally be essential to avoid shut contact with individuals who've a recognized parasitic an infection.
The treatment is on the market in pill type and is typically taken once as a single dose. It is necessary to observe the dosage instructions supplied by your physician or pharmacist and to complete the complete course of treatment. Failure to do so may end in incomplete elimination of the parasites, making the infection tougher to treat.
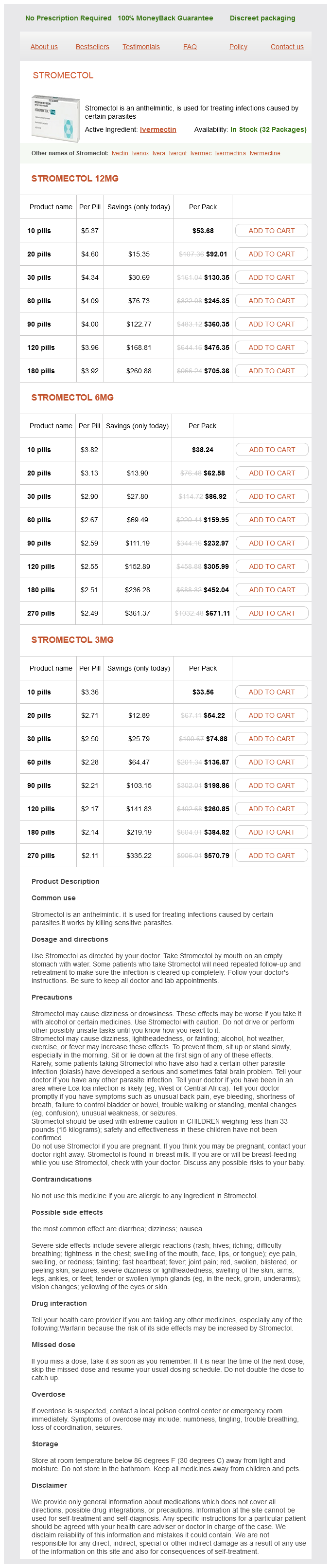
Revectina, also identified by its generic name Stromectol, is a drugs used for treating infections caused by sure parasites. It belongs to a class of medicine called anthelmintics, that are particularly designed to target and eliminate parasitic infections.
In conclusion, Revectina, also recognized as Stromectol, is a highly effective medication used within the remedy of parasitic infections. It works by paralyzing and finally killing the parasites, allowing the body to get rid of them naturally. It is essential to observe the dosage directions supplied by your doctor and to complete the total course of treatment for optimum efficacy. Proper hygiene and sanitation practices are also necessary in stopping parasitic infections. While the medication may have potential unwanted aspect effects, they are usually mild and well-tolerated. If you think you studied a parasitic infection, it is necessary to seek the advice of together with your doctor for correct diagnosis and therapy.
Revectina is generally well-tolerated, with only some reported side effects such as nausea, diarrhea, and dizziness. However, as with every medicine, some folks might experience extra severe side effects similar to allergic reactions, headache, and muscle aches. If you expertise any adverse reactions, you will want to converse with your physician immediately.
Revectina works by paralyzing and finally killing the parasites, permitting the body to naturally get rid of them. It is thought to have an impact on the parasite's nerve and muscle cells, interfering with their capacity to perform and survive throughout the host's physique.
Stromectol has been proven to be extremely efficient in treating a broad range of parasitic infections. It is particularly efficient in treating strongyloidiasis and onchocerciasis, two diseases attributable to roundworm and threadworm parasites, respectively.
In addition to its use in treating parasitic infections, Stromectol has also shown potential in treating different conditions, corresponding to rosacea, a skin situation characterized by redness and bumps on the face. It can be being studied for its potential to deal with different skin circumstances, corresponding to lice and scabies.
The effect appears to result popular antibiotics for sinus infection best purchase revectina, at least in part, from activation of 2 receptors in the lower brainstem region. Studies in knockout animals demonstrated the requirement for a functional 2 receptor for the hypotensive effect of clonidine. Clonidine also stimulates parasympathetic outflow, which may contribute to the slowing of heart rate as a consequence of increased vagal tone and diminished sympathetic drive. The drug has been used in the treatment of hypotensive states or off-label to relieve attacks of paroxysmal atrial tachycardia, particularly those associated with hypotension (see Chapter 30). This is advantageous in the treatment of patients with autonomic insufficiency and postural hypotension (McClellan et al. About half of an administered dose can be recovered unchanged in the urine; the t1/2 of the drug may increase with renal failure. A transdermal delivery patch permits continuous administration of clonidine as an alternative to oral therapy. The drug is released at an approximately constant rate for a week; 34 days are required to reach steady-state concentrations in plasma. When the patch is removed, plasma concentrations remain stable for about 8 h and then decline gradually over a period of several days; this decrease is associated with a rise in blood pressure. Clonidine is well absorbed after oral administration, with the t1/2 for elimination ranges from 12 to 24 h. Guanfacine and clonidine appear to have similar efficacy for the treatment of hypertension and a similar pattern of adverse effects. A withdrawal syndrome may occur after the abrupt discontinuation, but it is less frequent and milder than the syndrome that follows clonidine withdrawal; this difference may relate to the longer t1/2 of guanfacine. Tizanidine Tizanidine is a muscle relaxant used for the treatment of spasticity associated with cerebral and spinal disorders. Moxonidine also has analgesic activity, interacts synergistically with opioid agonists, and is used in treating neuropathic pain. The major adverse effects of clonidine are dry mouth and sedation, which may diminish in intensity after several weeks of therapy. About 15%20% of patients develop contact dermatitis when using the transdermal system. Cardiovascular System Apraclonidine Apraclonidine is a relatively selective 2 receptor agonist that is used topically to reduce intraocular pressure with minimal systemic effects. The drug also is used to control or prevent elevations in intraocular pressure that occur in patients after laser trabeculoplasty or iridotomy (see Chapter 69). Guanfacine is an 2 receptor agonist that is more selective than clonidine for 2 receptors. Cardiac output is not enhanced by therapeutic doses, and cerebral blood flow does not change much. The l-isomer is slightly more potent than the d-isomer in its cardiovascular actions. Other Smooth Muscles Brimonidine In general, smooth muscles respond to amphetamine as they do to other sympathomimetic amines. The contractile effect on the sphincter of the urinary bladder is particularly marked, and for this reason amphetamine has been used in treating enuresis and incontinence. The psychic effects depend on the dose and the mental state and personality of the individual. Performance of simple mental tasks is improved, but, although more work may be accomplished, the number of errors may increase. Many individuals given amphetamine experience headache, palpitation, dizziness, vasomotor disturbances, agitation, confusion, dysphoria, apprehension, delirium, or fatigue. In general, amphetamine prolongs the duration of adequate performance before fatigue appears, and the effects of fatigue are at least partly reversed, most strikingly when performance has been reduced by fatigue and lack of sleep. Such improvement may be partly due to alteration of unfavorable attitudes toward the task. However, amphetamine reduces the frequency of attention lapses that impair performance after prolonged sleep deprivation and thus improves execution of tasks requiring sustained attention. Amphetamine stimulates the respiratory center, increasing the rate and depth of respiration. In normal individuals, usual doses of the drug do not appreciably increase respiratory rate or minute volume. The site of action probably is in the lateral hypothalamic feeding center; injection of amphetamine into this area, but not into the ventromedial region, suppresses food intake. Hence, continuous weight reduction usually is not observed in obese individuals without dietary restriction. These mechanisms may have potential implications for neurotoxicity as well as dopaminergic neurodegenerative diseases (discussed further in the chapter). With still higher doses of amphetamine, disturbances of perception and overt psychotic behavior occur. The acute toxic effects of amphetamine usually are extensions of its therapeutic actions and as a rule result from overdosage. Confusion, aggressiveness, changes in libido, anxiety, delirium, paranoid hallucinations, panic states, and suicidal or homicidal tendencies occur, especially in mentally ill patients. Severe reactions have occurred with 30 mg, yet doses of 400500 mg are not uniformly fatal.
If the dosing interval t were chosen to be equal to the t1/2 best antibiotic for sinus infection cipro purchase revectina line, then the total fluctuation would be 2-fold; this is often a tolerable variation. If a drug is relatively nontoxic such that a concentration many times that necessary for therapy can be tolerated easily, the maximal dose strategy can be used, and the dosing interval can be much longer than the elimination t1/2 (for convenience). The minimal steady-state concentration Css, min may be reasonably determined by: C ss, min = F dose/Vss - kThe 1- e- kT (Equation 218) Dosing Interval for Intermittent Dosage Maintenance Dose In most clinical situations, drugs are administered in a series of repetitive doses or as a continuous infusion to maintain a steady-state concentration of drug associated with the therapeutic window. The term e-kThis the fraction of the last dose (corrected for bioavailability) that remains in the body at the end of a dosing interval. Thus, monitoring the clinical status of patients (new or increased ankle edema, inability to sleep in a recumbent position, decreased exercise tolerance), whether accomplished by home health follow-up or regular visits to the clinician, is essential to avoid untoward results (see Chapter 29). Maximum and minimum digoxin plasma concentrations then may be predicted depending on the dosage interval. If these terms are ignored for multiple oral dosing, one easily may estimate a maximal steady-state concentration by omitting the e-kT term in the numerator of Equation 218 (see Equation 219 in Box 25). Because of the approximation, the predicted maximal concentration from Equation 219 will be greater than that actually observed. When a constant dosage is given, reaching a steady-state drug level (the desired therapeutic concentration) will take four to five elimination half-times. This period can be too long when treatment demands a more immediate therapeutic response. In such a case, one can employ a loading dose, one or a series of doses given at the onset of therapy with the aim of achieving the target concentration rapidly. The loading dose is calculated as Loading dose = Target Cp · Vss/F (Equation 221) Thus, the plasma concentrations would fluctuate minimally about the steady-state concentration of 0. Arrhythmias encountered after myocardial infarction may be life threatening, and one cannot wait four half-times (48 h) to achieve a therapeutic concentration of lidocaine by infusion of the drug at the rate required to attain this concentration. Loading doses tend to be large, and they are often given parenterally and rapidly; this can be particularly dangerous if toxic effects occur as a result of actions of the drug at sites that are in rapid equilibrium with plasma. This occurs because the loading dose calculated on the basis of Vss subsequent to drug distribution is at first constrained within the initial and smaller "central" volume of distribution. It is therefore usually advisable to divide the loading dose into a number of smaller fractional doses that are administered over a period of time (Box 26). These two values can offer a more complete picture of the behavior of the drug in a specific patient (particularly if obtained over more than one dosing period) and can better support pharmacokinetic modeling to adjust treatment. When constant dosage is given, steady state is reached after four to five elimination half-times. Yet, for toxic drugs, if sampling is delayed until steady state, the damage may have been done. In such cases, the first sample should be taken after two t1/2 assuming that no loading dose has been given. If the concentration already exceeds 90% of the eventual expected mean steady-state concentration, the dosage rate should be halved, another sample obtained in another two (supposed) t1/2, and the dosage halved again if this sample exceeds the target. Practical details associated with therapeutic drug monitoring should be kept in mind. Early postabsorptive concentrations do not reflect clearance; they are determined primarily by the rate of absorption, the "central" (rather than the steady-state) volume of distribution, and the rate of distribution, all of which are pharmacokinetic features of virtually no relevance in choosing the long-term maintenance dosage. When the goal of measurement is adjustment of dosage, the sample should be taken just before the next planned dose, when the concentration is at its minimum. Patient outcomes within schizophrenia treatment: a look at the role of long-acting injectable antipsychotics. Racial/ethnic differences in drug disposition and response: review of recently approved drugs. Complications after unintentional intra-arterial injection of drugs: risks, outcomes, and management strategies. Therefore, the ratio between the measured and desired concentrations can be used to adjust the dose, consistent with available dosage sizes: C ss (measured) Dose (previous) = C ss (predicted) Dose (new) (Equation 223) Consider the previously described patient given 0. The effects of most drugs result from their interaction with macromolecular components of the organism. The term drug receptor or drug target denotes the cellular macromolecule or macromolecular complex with which the drug interacts to elicit a cellular or systemic response. Going far beyond the traditional concept of a drug are genetically modified viruses and microbes. One recently approved agent for treating melanoma is a genetically modified live oncolytic herpes virus that is injected into tumors that cannot be removed completely by surgery. Agents that are only partially as effective as agonists are termed partial agonists. In the presence of a full agonist, partial and inverse agonists will behave as competitive antagonists. Specificity of Drug Responses the strength of the reversible interaction between a drug and its receptor, as measured by the dissociation constant, is defined as the affinity of one for the other. Conversely, a drug acting on a receptor expressed ubiquitously throughout the body will exhibit widespread effects. Many clinically important drugs exhibit a broad (low) specificity because they interact with multiple receptors in different tissues. One example of a drug that interacts with multiple receptors is amiodarone, an agent used to treat cardiac arrhythmias. A drug may have Physiological Receptors Many drug receptors are proteins that normally serve as receptors for endogenous regulatory ligands.
Revectina Dosage and Price
Stromectol 12mg
- 10 pills - $53.68
- 20 pills - $92.01
- 30 pills - $130.35
- 60 pills - $245.35
- 90 pills - $360.35
- 120 pills - $475.35
- 180 pills - $705.36
Stromectol 6mg
- 10 pills - $38.24
- 20 pills - $62.58
- 30 pills - $86.92
- 60 pills - $159.95
- 90 pills - $232.97
- 120 pills - $305.99
- 180 pills - $452.04
- 270 pills - $671.11
Stromectol 3mg
- 10 pills - $33.56
- 20 pills - $54.22
- 30 pills - $74.88
- 60 pills - $136.87
- 90 pills - $198.86
- 120 pills - $260.85
- 180 pills - $384.82
- 270 pills - $570.79
Verapamil in the prophylaxis of episodic cluster headache: a double-blind study versus placebo antibiotics kinds trusted 12 mg revectina. A secondary goal is to discuss vestibular abnormalities such as the superior canal dehis cence, vestibular paroxysmia, and the simultaneous acute and chronic bilateral vestibular loss syndromes that have become better understood in the last decade. By virtue of their symptoms these patients frequently visit the neuro logist as the initial specialist or in expert consultation. Definition · Vertigo: a spontaneous pathologic perception of spinning or tilting that builds up over a time period ranging from seconds to minutes, and is the result of an acute peripheral or central vestibulopathy, typically occurring spontaneously and potentially exacerbated by motion. Recent clinical epidemiologic data support the concept that the type of sensation described by the patient may be potentially misleading, when it is intermittent, timing (duration) of the episode, and triggers are more relevant for proper syndrome classification. Tip E the subjective description of the terms listed above may be quite variable; therefore, an emphasis on the triggers for a specific complaint and duration of symptoms may prove more efficient. Vertigo 157 Classification according to timing Table 19 presents the classification of vertigo on the basis of timing (duration). Episodic disequilibrium and presyncope with or without a sensation of rotation may occur with nonvestibular pathology, in particular orthostatic hypotension and other cardiovascular disorders and endocrine disorders. Stroke, affecting the labyrinth, vestibular nerve, brainstem vestibular pathways, and cerebellum, can cause either pseudolabyrinthitis or pseudoneuritis, depending on whether hearing is affected or spared. Generally speaking, complete unilateral vestibular periphery or central lesions compensate in a matter of a few weeks; typically, the acute symptoms subside and are generally superseded by a sensation of unsteadiness and visual blurring with rapid gaze shifts or head movement. Epidemiology Dizziness is a frequent complaint in both acute emergency and neurologic practice. Given this epidemiologic picture, clinicians evaluating patients with dizziness confront a spectrum of disorders that vary in prognosis from benign to potentially life threatening. A practical algorithm for the diagnosis and management of vertiginous patients is suggested (146, next page). Examination involves assessment of sitting posture, followed by standing in a comfortable position or with a wide base. Imbalance; falls Romberg test Positive sway or fall to and fro Positive sway or fall to side Position sense normal Position sense abnormal Head impulse test horizontal Horizontal nystagmus · Cerebellar vermis lesions · Association with brainstem lesions causing up- and downbeat nystagmus · Positional vertigo · Thalamic lesion Neuropathy Positive Negative Unidirectional; increasing in the dark Bidirectional horizontal nystagmus Peripheral vestibulopathy; lateral pons Cerebellar stroke; brainstem stroke Peripheral vestibular lesion Brainstem root entry zone Rarely cerebellar lesion Cerebellar lesion Brainstem lesion Etiology and pathophysiology the study of the otopathology of vertigo has been complicated by the fact that the membranous labyrinth is housed within the bony labyrinth inside the temporal bone, and the preparation of the pathology specimen for examination involves a complicated lengthy process. In a few patients with atherosclerotic disease of the vertebrobasilar system, pathologic evidence of ischemic infarction of the labyrinth and cochlea has been demonstrated9. Pathologic evidence of simultaneous infarction of the labyrinth and the lateral brainstem has been previ ously reported9. After reaching the supine head hanging position with a delay of few seconds, an intense spinning sensa tion occurs with pronounced transient nystagmus. Vestibular paroxysmia Episodic vertigo as a result of compression of the vestibu lar nerve by an arterial vascular structure is analogous to a common neurovascular compression syndrome such as trigeminal neuralgia or hemifacial spasm. In current clinical practice, gentamicin ranks at the top of the list of drug toxicities. Associated symptoms may include hearing impairment, tinnitus, nausea, vomit ing and profuse sweating, inability to maintain sitting or standing balance or to do tandem gait, falls, oscillopsia, diplopia and, at times with central lesions, other neuro logic symptoms. Fol lowing posture testing if normal, regular gait, tandem gait, and the Fukuda step tests are assessed. The direc tion of fall during these postural tests may be ipsi or contralesional, depending on localization. E the direction of fall may be ipsi- or contralesional, consequently it does not lateralize the lesion localization. Nystagmus type assessment Spontaneous fixation and eccentric lateral and vertical gaze nystagmus is tested first in light and subsequently in dark, using either Frenzel or videogoggles, and the nys tagmus type provides localizing information. Tips E the evaluation of nystagmus direction (fast phases) in primary gaze is a useful tool in the classification of vestibular disorders. E Vertical nystagmus is almost always due to a central lesion or an altered central mechanism. However, the latter tests may infrequently be positive in vestibular root entry zone lesions involving the lateral pons. This sign is the result of an acute unilateral deficiency of the otolithocular reflex. Additional findings included inability to sit at the bedside without support due to right lateropulsion. In this case the head tilt and the conjugate ocular deviation toward the right shoulder are shown. On the basis of the examination, a central vestibular pathway lesion was suspected and imaging ordered. Additional bedside evaluation Hearing can be tested with finger rubbing, and the tra ditional Weber and Rinne signs should also be tested. There is a brief latency of 30 seconds, and vertigo does not last more than 30 seconds. The patients do not have symptoms while sitting comfortably upright and their examination shows no evidence of nystagmus. An upbeat, torsional nystagmus directed toward the dependent ear is the most common response (pos terior semicircular canalolithiasis), and the nystagmus subsides 30 seconds later. Additional vestibular laboratory testing Caloric and rotational testing in these circumstances may detect diagnostic abnormalities. The direction of the nystagmus cannot be used for localization as it depends on the stage of the attack and can be contralesional (paretic) in the early attack phase or ipsilesional (recovery) in the late attack phase. Observe conjugate deviation of the eyes to the left in an 18-year-old, previously healthy female with an acute vestibular syndrome. On the basis of this examination, a central lesion in the left lateral brainstem or the cerebellum was suspected and imaging was obtained. It is very helpful in patients with bilateral vestibular ototoxicity, in combined central/ peripheral lesions, and in central lesions in which quantitative oculomotor tests could detect subtle deficiencies. The patient underwent surgery with repair of the dehiscence and clinical improvement.