General Information about Topiramate
Topiramate is on the market in pill and capsule varieties, and the dosage varies depending on the situation being treated, the patient's age, weight, and underlying well being conditions. It is normally taken twice a day, with or with out meals. In some cases, the dosage could additionally be elevated gradually until the specified impact is achieved. It is essential to comply with the dosage directions supplied by the physician fastidiously. Abruptly stopping the treatment may cause a rise in seizures or other withdrawal symptoms.
Like any other treatment, Topiramate has its potential unwanted effects that can vary from mild to extreme. Some of the widespread unwanted side effects include dizziness, drowsiness, fatigue, decreased appetite, nausea, and weight loss. In some instances, sufferers could expertise extra extreme side effects corresponding to imaginative and prescient issues, confusion, mood adjustments, or issue concentrating. It is essential to report any uncommon side effects to the physician instantly.
Topiramate, commonly often identified as Topamax, is a medication used to deal with seizures in patients with sure neurological conditions. It is a broadly prescribed prescription drug that has been used to successfully management seizures for over 20 years. In addition to its major use in treating seizures, Topiramate has additionally been permitted for other makes use of such as migraine prevention and weight reduction.
Topiramate belongs to a category of medication called anticonvulsants, which work by decreasing the abnormal electrical exercise within the mind that may lead to seizures. It does this by enhancing the exercise of the neurotransmitter gamma-aminobutyric acid (GABA) in the mind. GABA is liable for inhibiting excessive exercise between nerve cells, and by increasing its activity, Topiramate helps to settle down the overexcited mind cells that lead to seizures.
In conclusion, Topiramate has been a game-changer within the remedy of seizures. It is a well-tolerated medicine that has helped tens of millions of sufferers worldwide to successfully manage their seizures and improve their high quality of life. With its extra makes use of in preventing migraines and aiding weight reduction, Topiramate has proven to be a useful treatment in the healthcare industry. However, it is important to use it as directed and underneath the supervision of a health care provider to make sure its security and effectiveness. If you or a liked one are affected by seizures, make certain to consult with a healthcare skilled to see if Topiramate is an acceptable option.
This medicine is mainly prescribed to treat partial-onset seizures, that are the most typical kind of seizures in adults. It can additionally be used to treat several different kinds of seizures, together with main generalized tonic-clonic seizures, Lennox-Gastaut syndrome, and seizures associated with a rare genetic dysfunction known as Dravet syndrome. Topiramate just isn't a remedy for seizures, however it could effectively management and stop seizures from occurring.
Apart from its primary use in treating seizures, Topiramate has been permitted for other makes use of as well. It has been found to be efficient in stopping migraine headaches. It works by lowering the frequency and severity of migraine assaults by targeting a unique neurotransmitter, glutamate, which is concerned within the transmission of ache alerts. Topiramate may assist sufferers affected by weight problems to lose weight. Studies have shown that it can cut back urge for food and increase the sensation of feeling full, leading to weight reduction.
Topiramate might work together with other drugs, nutritional vitamins, or natural dietary supplements. It is essential to inform the doctor of another medicines being taken to prevent potential interactions. It is also not beneficial for pregnant or breastfeeding ladies, as it can cause hurt to the infant.
Each of these can help to slow virus multiplication and prevent liver damage in many but not all patients treatment modality definition purchase topiramate toronto. Hepatitis C Virus Hepatitis C is sometimes referred to as the "silent epidemic" because 3. The jaundice that is typical of other forms of hepatitis is not seen in hepatitis E infection. Pregnant women in their third trimester are at highest risk for this severe form of disease, and the fatality rate is nearly 20%. A majority of the cases reported in the United States occur in people who have traveled to these endemic regions. Hepatitis E virus is transmitted by the fecal-oral route, mainly through contaminated water and food. The infection does not seem to be transmitted from person to person, though blood transfusions have been documented to transmit the pathogen to uninfected patients. It shares many characteristics of hepatitis B disease, but it is much more likely to become chronic. Pathogenesis and Virulence Factors the virus is so adept at establishing chronic infections that researchers are studying the ways that it evades immunologic detection and destruction. List the possible causative agents for the following infectious gastrointestinal conditions: dental caries, periodontal diseases, mumps, and gastric ulcers. Differentiate among the main types of hepatitis and discuss causative agents, modes of transmission, diagnostic techniques, prevention, and treatment of each. It is more commonly transmitted through blood contact (both "sanctioned," such as in blood transfusions, and "unsanctioned," such as needle sharing by injecting drug users) than through transfer of other body fluids. Anyone with a history of exposure to blood products or organs before 1992 (when effective screening became available) is at higher risk for this infection, as is anyone with a history of injecting drug use. It has a very high prevalence in parts of South America, Central Africa, and China. Although they can cause symptoms that may be mistaken for some of the diseases discussed elsewhere in this chapter, helminthic diseases are usually and Treatment There is currently no vaccine for hepatitis C. Helminthic infection usually provokes an increase in granular leukocytes called eosinophils, which have a specialized capacity to destroy multicellular parasites. This increase, termed eosinophilia, is a hallmark of helminthic infection and is detectable in blood counts. If the following symptoms occur coupled with eosinophilia, helminthic infection should be suspected. Many of these infections are considered "neglected tropical infections"-infections that cast a large burden of disease in the poorest countries of the world yet receive the least recognition and research funding today (Insight 22. Due to the efforts of dedicated tropical disease medicine specialists and organizations, such as both the Carter and the Gates Foundations, some of these helminthic diseases are on the decline. Helminthic infections may be acquired through the fecal-oral route or through penetration of the skin, but most of them spend part of their lives in the intestinal tract. While the worms are in the intestines, they can produce a gamut of intestinal symptoms. Some of them also produce symptoms outside of the intestine; they are considered in separate categories. We talk about diagnosis, pathogenesis and prevention, and treatment of the helminths as a group in the next subsections. Pathogenesis and Virulence Factors in General General Clinical Considerations Up to this point, the diseases in this book have been arranged in the same way, based on how the disease appears in terms of signs Helminths have numerous adaptations that allow them to survive in their hosts. They have specialized mouthparts for attaching to tissues and for feeding, enzymes with which they liquefy and penetrate tissues, and a cuticle or other covering to protect them from host defenses. In addition, their organ systems are usually reduced to the essentials: getting food and processing it, moving, and reproducing. If this is the case, the host in which the adult worm reproduces sexually is called the definitive host (usually a vertebrate). Sometimes the actual definitive host is not the host usually used by the parasite but an accidental bystander. Humans often become the accidental definitive hosts for helminths whose normal definitive host is a cow, pig, or fish. Helminths may require no intermediate host at all or may need one or more intermediate hosts for their entire life cycle. Or maybe it is easier to stomach because we are confident that protozoal and helminthic infections are relatively rare in the United States. These diseases can affect anyone, but in the United States they are much more likely to be found in residents of poor neighborhoods and in immigrants from countries in which the diseases are prevalent. One of the consequences of that circumstance is that it is difficult to estimate infection rates, but new attempts have begun. Up to 300,000 people in the United States are currently infected with the protozoan that causes Chagas disease. A differential blood count showing eosinophilia and serological tests indicating sensitivity to helminthic antigens all provide indirect evidence of worm infection. A history of travel to the tropics or immigration from those regions is also helpful, even if it occurred years ago, because some flukes and nematodes persist for decades. The most definitive evidence, however, is the discovery of eggs, larvae, or adult worms in stools or in tissues. The worms are sufficiently distinct in morphology that positive identification can be based on any stage, including eggs. Stool is commonly examined in a microscopic procedure called "an O & P," or an ova and parasite smear. That said, not all of these diseases result in eggs or larval stages that can easily be found in stool. No vaccines are available to prevent any of the helminthic infections described here.
The mammary glands of the breasts lie within the subcutaneous tissue of the thoracic wall symptoms rabies order generic topiramate online. The anterolateral axioappendicular muscles (see Chapter 3, Upper Limb) that overlie the thoracic cage and form the bed of the breast are encountered in the thoracic wall and may be considered part of it but are distinctly upper limb muscles based on function and innervation. The domed shape of the thoracic cage provides remarkable rigidity, given the light weight of its components, enabling it to perform the following functions: 720 Protect vital thoracic and abdominal organs (most air or fluid filled) from external forces. Resist the negative (subatmospheric) internal pressures generated by the elastic recoil of the lungs and inspiratory movements. Provide the anchoring attachment (origin) of many of the muscles that move and maintain the position of the upper limbs relative to the trunk, as well as provide the attachments for muscles of the abdomen, neck, back, and respiration. Although the domed shape of the thoracic cage provides rigidity, its joints and the thinness and flexibility of the ribs allow it to absorb external blows and compressions without fracture and to change its shape for respiration. Because the most important structures within the thorax (heart, great vessels, lungs, and trachea), as well as its floor and walls, are constantly in motion, the thorax is one of the most dynamic regions of the body. With each breath, the muscles of the thoracic wall, working in concert with the diaphragm and muscles of the abdominal wall, vary the volume of the thoracic cavity. This is accomplished first by expanding the capacity of the cavity, thereby causing the lungs to expand and draw air in, and then, due to lung elasticity and muscle relaxation, decreasing the volume of the cavity and causing them to expel air. The ribs and costal cartilages form the largest part of the thoracic cage; both are identified numerically, from the most superior (1st rib or costal cartilage) to the most inferior (12th). Each rib has a spongy interior containing bone marrow (hematopoietic tissue), which forms blood cells. True (vertebrosternal) ribs (1st7th ribs): They attach directly to the sternum through their own costal cartilages. False (vertebrochondral) ribs (8th, 9th, and usually 10th ribs): Their cartilages are connected to the cartilage of the rib above them; thus, their connection with the sternum is indirect. Floating (vertebral, free) ribs (11th, 12th, and sometimes 10th ribs): the rudimentary cartilages of these ribs do not connect even indirectly with the 722 sternum; instead, they end in the posterior abdominal musculature. Body (shaft): thin, flat, and curved, most markedly at the costal angle where the rib turns anterolaterally. The concave internal surface of the body has a costal groove paralleling the inferior border of the rib, which provides some protection for the intercostal nerve and vessels. T1 has a vertebral foramen and body similar in size and shape to a cervical vertebra. The planes of the articular facets of thoracic vertebrae define an arc (red arrows) that centers on an axis traversing the vertebral bodies vertically. Superior and inferior costal facets (demifacets) on the vertebral body and costal facets on the transverse processes. It has a single facet on its head for articulation with T1 vertebra only and two transversely directed grooves crossing its superior surface for the subclavian vessels. The grooves are separated by a scalene tubercle and ridge, to which the anterior scalene muscle is attached. The 2nd rib has a thinner, less curved body and is substantially longer than the 1st rib. Its head has two facets for articulation with the bodies of the T1 and T2 vertebrae; its main atypical feature is a rough area on its upper 725 surface, the tuberosity for serratus anterior, from which part of that muscle originates. The 10th12th ribs, like the 1st rib, have only one facet on their heads and articulate with a single vertebra. Costal cartilages prolong the ribs anteriorly and contribute to the elasticity of the thoracic wall, providing a flexible attachment for their anterior ends (tips). The cartilages increase in length through the first 7 and then gradually decrease. The 11th and 12th costal cartilages form caps on the anterior ends of the corresponding ribs and do not reach or attach to any other bone or cartilage. The costovertebral joints include the joint of head of rib, in which the head articulates with two adjacent vertebral bodies and the 726 intervertebral disc between them, and the costotransverse joint, in which the tubercle of the rib articulates with the transverse process of a vertebra. The rib moves (elevates and depresses) around an axis that traverses the head and neck of the rib (arrows). The spaces are named according to the rib forming the superior border of the space-for example, the 4th intercostal space lies between ribs 4 and 5. Intercostal spaces are occupied by intercostal muscles and membranes, and two sets (main and collateral) of intercostal blood vessels and nerves, identified by the same number assigned to the space. The space below the 12th rib does not lie between ribs and thus is referred to as the subcostal space, and the anterior ramus (branch) of spinal nerve T12 is the subcostal nerve. The spaces widen further with inspiration and on contralateral extension and/or lateral flexion of the thoracic vertebral column. Characteristic features of thoracic vertebrae include the following: Bilateral costal facets (demifacets) on the vertebral bodies, usually occurring in inferior and superior pairs, for articulation with the heads of ribs. Costal facets on the transverse processes for articulation with the tubercles of ribs, except for the inferior two or three thoracic vertebrae. Superior and inferior costal facets, most of which are small demifacets, occur as bilaterally paired, planar surfaces on the superior and inferior posterolateral margins of the bodies of typical thoracic vertebrae (T2T9). Atypical thoracic vertebrae bear whole costal facets in place of demifacets: the superior costal facets of vertebra T1 are not demifacets because there are no demifacets on the C7 vertebra above, and rib 1 articulates only with vertebra T1. T10 has only one bilateral pair of (whole) costal facets, located partly on its body and partly on its pedicle.
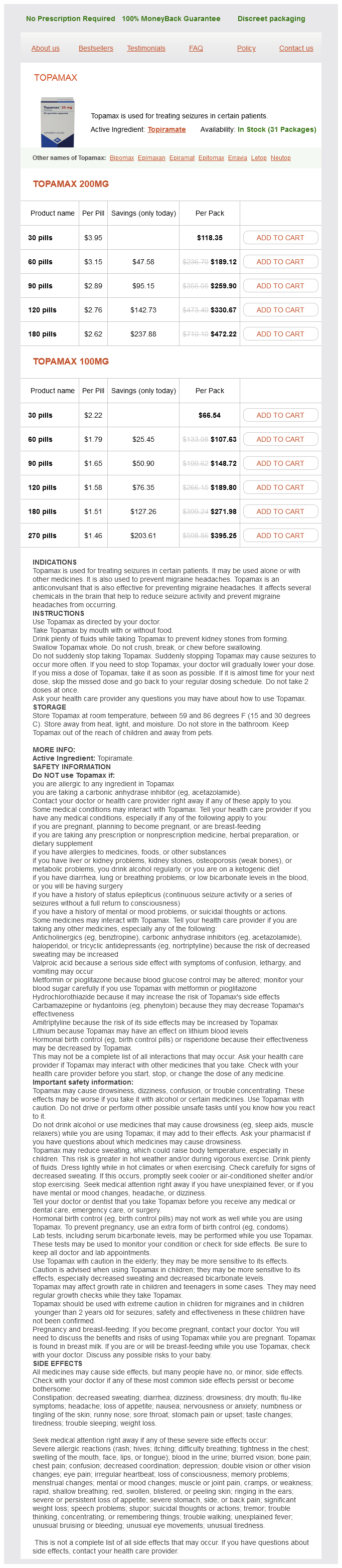
Topiramate Dosage and Price
Topamax 200mg
- 30 pills - $118.35
- 60 pills - $189.12
- 90 pills - $259.90
- 120 pills - $330.67
- 180 pills - $472.22
Topamax 100mg
- 30 pills - $66.54
- 60 pills - $107.63
- 90 pills - $148.72
- 120 pills - $189.80
- 180 pills - $271.98
- 270 pills - $395.25
The branches of the 779 intercostal nerves convey sensory fibers from the skin of the breast and sympathetic fibers to the blood vessels in the breasts and smooth muscle in the overlying skin and nipple administering medications 7th edition topiramate 100 mg buy overnight delivery. They can be palpated easily throughout their length, especially where their medial ends articulate with the manubrium of the sternum. The clavicles demarcate the superior division between zones of lymphatic drainage: above the clavicles, lymph flows ultimately to inferior jugular lymph nodes; below them, parietal lymph (that from the body wall and upper limbs) flows to the axillary lymph nodes. The sternum (breast bone) lies subcutaneously in the anterior median line and is palpable throughout its length. Between the prominences of the medial ends of the clavicles at the sternoclavicular joints, the jugular notch in the manubrium can be palpated between the prominent medial ends of the clavicles. The notch lies at the level of the inferior border of the body of T2 vertebra and the space between the 1st and 2nd thoracic spinous processes. The sternal angle is palpable and often visible in young people because of the slight movement that occurs at the manubriosternal joint during forced respiration. The xiphisternal joint is palpable and is often seen as a ridge, at the level of the inferior border of T9 vertebra. The costal margins, formed by the joined costal cartilages of the 7th10th ribs, are easily palpable because they extend inferolaterally from the xiphisternal joint. The ribs and intercostal spaces provide a basis for locating or describing the position of structures or sites of trauma or pathology on or deep to the thoracic wall. Because the 1st rib is not palpable, rib counting in physical examinations starts with the 2nd rib adjacent to the subcutaneous and easily palpated sternal angle. To count the ribs and intercostal spaces anteriorly, slide the fingers (digits) laterally from the sternal angle onto the 2nd costal cartilage and begin counting the ribs and spaces by moving the fingers from here. The 1st intercostal space is that superior to the 2nd costal cartilage-that is, intercostal spaces are numbered according to the rib forming their superior boundary. Generally, it is more reliable to count intercostal spaces, since the fingertip tends to rest in (slip into) the gaps between the ribs. If the fingers are removed from the thoracic wall while counting spaces, the finger may easily be returned to the same space, mistaking it for the one below. While the ribs and/or intercostal spaces provide the "latitude" for navigation and localization on the thoracic wall, several imaginary lines facilitate anatomical and clinical descriptions by providing "longitude. Additional lines (not illustrated) are extrapolated along the borders of palpable bony formations, such as the parasternal and paravertebral lines (G. Breasts are the most prominent surface features of the anterior thoracic wall, especially in women. The inferior ribs and costal margins are often apparent, especially when the abdominal muscles are contracted. The intercostal musculature is not normally evident; however, in (rare) cases in which there is an absence or atrophy of the intercostal musculature, the intercostal spaces become apparent with respiration: during inspiration, they are concave; during expiration, they protrude. The female breasts vary in the size, shape, and symmetry-even in the same person. The areola usually darkens during pregnancy and retains the darkened pigmentation thereafter. The areola is normally dotted with the papular (small elevated) openings of the areolar glands (sebaceous glands in the skin of the areola). On occasion, one or both nipples are inverted (retracted); this minor congenital anomaly may make breastfeeding difficult. Usually, however, the position of nipples varies considerably with breast size, especially in multiparous women- those who have given birth to two or more children. Consequently, because of variations in size and shape, the nipples are not a reliable guide to the 4th intercostal spaces in adult females. Although mammary glands are prepared for secretion by midpregnancy, they do not produce milk until shortly after the baby is born. Colostrum, a creamy white to yellowish premilk fluid, may secrete from the nipples during the last trimester of pregnancy and during initial episodes of nursing. In multiparous women (those who have given birth two or more times), the breasts often become large and pendulous. The breasts in elderly women are usually small because of the decrease in fat and the atrophy of glandular tissue. Carcinoma of the Breast Understanding the lymphatic drainage of the breasts is of practical importance in predicting the metastases (dispersal) of cancer cells from a carcinoma of the breast (breast cancer). Metastatic cancer cells that enter a lymphatic vessel usually pass through two or three groups of lymph nodes. Interference with dermal lymphatics by cancer may cause lymphedema (edema, excess fluid in the subcutaneous tissue) in the skin of the breast, which in turn may result in deviation of the nipple and a thickened, leather-like appearance of the skin. Larger dimples (fingertip size or bigger) result from cancerous invasion of the glandular tissue and fibrosis (fibrous degeneration), which causes shortening or places traction on the suspensory ligaments. Subareolar breast cancer may cause retraction of the nipple by a similar mechanism involving the lactiferous ducts. Breast cancer typically spreads from the breast by means of lymphatic vessels (lymphogenic metastasis), which carry cancer cells from the breast to the lymph nodes, chiefly those in the axilla. Because most of lymphatic drainage of the breast is to the axillary lymph nodes, they are the most common site of metastasis from a breast cancer. Enlargement of these palpable nodes suggests the possibility of breast cancer and may be key to early detection. However, the absence of enlarged axillary lymph nodes is no guarantee that metastasis from a breast cancer has not occurred; the malignant cells may have passed to other nodes, such as the infraclavicular and 788 supraclavicular lymph nodes or directly into the systemic circulation.