General Information about Toradol
It can be essential to note that Toradol should not be used in sure situations, such as by individuals with a historical past of allergic reactions to aspirin or different NSAIDs, these with a historical past of bleeding issues, and pregnant ladies. It can also work together with different drugs, so it's essential for patients to reveal all medicines they are taking to their healthcare supplier.
Despite its effectiveness, Toradol does come with potential unwanted effects. These embrace nausea, vomiting, stomach pain, dizziness, and drowsiness. In rare instances, it might possibly also result in more severe circumstances such as heart attack, stroke, or liver injury. For this cause, it is necessary for patients to discuss their medical history and another drugs they are taking with their physician earlier than beginning Toradol.
One of the primary advantages of Toradol is its capacity to offer strong pain relief. It works by inhibiting the manufacturing of prostaglandins, that are chemical compounds that cause inflammation and contribute to pain. This makes it a extremely efficient possibility for treating reasonable to extreme ache that's not responding to over-the-counter pain relievers.
Toradol is often used in hospital settings after surgeries or procedures, as it provides fast and effective ache reduction. In addition, it might be administered through an intramuscular or intravenous injection, making it a super option for patients who are unable to take medicine orally.
First approved by the United States Food and Drug Administration (FDA) in 1989, Toradol is out there in both oral and injectable forms. It is often seen as a preferable different to opioids as a end result of its lower potential for habit and abuse. However, it is important to note that like all medicines, Toradol does come with its personal set of dangers and side effects.
Another benefit of Toradol is its short-term use. It is usually prescribed for no more than 5 days, lowering the risk of long-term unwanted effects similar to gastrointestinal bleeding and kidney damage. This also helps to stop sufferers from becoming dependent on the treatment for ache administration.
In conclusion, Toradol is a robust and efficient treatment for the short-term therapy of reasonable to extreme pain. Its use is limited to 5 days or less, reducing the chance of long-term side effects. However, like all medicines, it's important for patients to inform their doctor about any medical circumstances or different medications they're taking to make sure protected and effective use of Toradol.
Toradol, additionally known by its generic name ketorolac, is a nonsteroidal anti-inflammatory drug (NSAID) that's primarily used for the remedy of average to extreme pain. It is often prescribed for the short-term relief of ache following surgical procedure or from conditions similar to kidney stones, migraine complications, and osteoarthritis.
Lesions usually heal without scarring arizona pain treatment center gilbert buy toradol 10 mg low cost, but secondarily infected lesions may require antibiotic therapy. Identification and elimination of the habit is necessary for resolution of habit-related lesions. In this radiograph the condyles bend inward at nearly 90 degrees above the fracture lines. Patients undergoing chemotherapy are encouraged to brush two or three times per day with a soft bristle toothbrush. If a patient develops oral mucositis, chlorhexidine may need to be discontinued because its high alcohol content may dehydrate the tissue. It is also important for patients undergoing chemotherapy to supplement fluoride because of the possibility of xerostomia (dry mouth), which may lead to increased caries risk. Trauma to the Dentition As noted earlier, facial injuries in childhood frequently involve the dentition and supporting bones. One prospective study showed that 50% of children had suffered at least one dental injury by age 14. Although falls are the major source in early childhood, bicycle and skateboard accidents, contact sports, fights, and motor vehicle accidents become more prevalent with advancing age. The risk of facial injuries is relatively high in (1) children with neurologic disorders that impair coordination; (2) children with protruding maxillary anterior teeth; (3) children with a deviant anatomic relationship, such as an anterior open bite or a hypoplastic upper lip; and (4) 2- to 3-year-old children with immature motor skills and coordination. Falling while a child is actively using a bottle, sippy cup, or pacifier is associated with more traumatic dental injuries. A, A large gaping tongue laceration in a toddler produced by the upper front teeth being forced through the tissue by a fall with the tongue protruded. B, this small laceration, although gaping slightly, does not require surgical closure. In this site, delayed hemorrhage after separation of the eschar and deformity with scarring are particular problems. Potential Complications Pulp hemorrhage and/or vasodilation of the pulp vessels are a common response to concussive injury to a tooth and can lead to development of discoloration within 10 to 14 days. Excessive pulpal vasodilation can actually result in pressure necrosis of the pulp. Injuries that produce loosening or displacement of a tooth disrupt the anchoring periodontal ligament. If disruption is mild, there may be no sequelae, although in some cases it stimulates overactive bony repair, ankylosing the tooth in place. When disruption is more severe, the neurovascular bundle can be torn, resulting in pulpal necrosis, which then may lead to abscess formation. Finally, dental fractures in which dentin and/or pulp are exposed open a pathway for bacteria and may lead to abscess formation. Several extensive classifications of tooth injuries have been suggested, but for the purpose of this text a more simplified descriptive classification is presented. However, any fracture of the crown that results in exposure of the dentin requires emergency treatment to prevent infection and subsequent pulp necrosis. The treatment of choice is to seal the exposed dentin with calcium hydroxide and protect it with an acid-etched resin bandage. As noted earlier, dental fragments are occasionally embedded in the soft tissues of the lip or tongue; therefore appropriate examination and palpation of these areas are indicated. Crown Fractures With Pulpal Exposure Fractures that traverse all three tooth layers to expose the pulp usually involve a significant loss of tooth structure. On physical examination, the fracture surface reveals the pink central pulp surrounded by the beige dentinal layer. Severe vertical or diagonal fractures may also result in pulp exposure and can at times extend to involve the root. Such teeth must be treated on an emergency basis by pulp capping, pulpotomy, or root canal therapy, depending on severity. Crown Craze or Crack A significant number of children are discovered during routine physical examination to have "cracks" in the enamel of their teeth. Such cracks are presumably caused by relatively minor trauma or temperature changes. Root Fractures Root fractures are less common in the primary dentition; and when they occur, they usually require no therapy. If the coronal segment represents an aspiration risk or the patient has traumatic occlusion, the treatment of choice is extraction of the primary tooth. Root fractures of permanent teeth may occur with or without loss of crown structure and may be asymptomatic. If a seemingly normal tooth is tender or exhibits increased mobility after trauma, root fracture should be suspected and radiographs obtained. In general the prognosis is good, and treatment may include splinting the involved segment, with or without root canal therapy. If the root fracture is in the coronal third of the tooth, splinting may be recommended for up to 4 months. Displacement Injuries Displacement injuries result in extrusion, intrusion, or lateral displacement (labially or lingually) and are most commonly seen in the primary dentition, where the combination of a short root length and a "pliable" bony structure seems to permit displacement to occur. Displacement injuries are often the cause of significant discomfort, bleeding, and possible interference with mastication and occlusion. Further, being the result of moderate to severe mechanisms of injury, fractures of underlying bony structures are common associated findings.
The latter include congenital vertebral anomalies pain treatment in multiple myeloma order toradol 10 mg visa, a spinal growth disturbance known as Scheuermann disease. Patients with a structural deformity may complain of backache aggravated by motion. Evaluation of the effects of Herniated Intervertebral Disk Although relatively common in adults, herniated disks occur only rarely in children and infrequently in adolescents. The angle of measurement (here, 75 degrees) is determined by the intersection of lines drawn perpendicular to the vertebrae at the ends of the curve (Cobb method). Patients often describe a peculiar "pulling" sensation in a lower extremity or liken their pain to a "toothache" in the distribution of the L5 or S1 nerve roots (see Chapter 16). Forward flexion, sitting, coughing, and straining aggravate the neurologic symptoms. On examination, an antalgic scoliosis of the lumbar spine may be apparent, which the patient is unable to reduce. Inability to reverse the normal lumbar lordosis is noted, and symptoms may be aggravated by attempts at flexion. The straight leg raising test is often positive (radicular symptoms being reproduced when the limb is raised by the examiner; see the Thoracolumbar Spine section, earlier, and. The differential diagnosis may include hematogenous disk space infection or vertebral osteomyelitis, spinal cord or neural element tumor, and spondylolisthesis with nerve root irritation. Nonsurgical treatment consisting of rest and anti-inflammatory agents may be successful, but if a profound neurologic deficit is present or if incapacitating symptoms persist, surgical disk excision may be indicated. A, the patient is attempting to correct the deformity, but because of its fixed nature, he cannot do so and must compensate for this with an increased lumbar lordosis. B, this tomographic cut shows anterior wedging of three consecutive vertebral bodies and clearly demonstrates the associated erosion of the vertebral end plates and Schmorl nodules. To stand upright, the patient must increase his lumbar lordosis and thrust his head forward to center it above the pelvis. C, Radiographically, the vertebral wedging that underlies the kyphotic deformity is evident. The forward slippage of L5 on the sacrum was the result of a fatigue fracture of the pars interarticularis. B, In the lateral view, the torso is thrust forward, the buttocks are flattened, and there are flexion deformities of the hips and knees. C, the L5 vertebra has completely translocated off the sacrum as the result of a congenital insufficiency of the posterior elements; the lumbar spine has essentially migrated anteriorly and into the pelvis. A, Diskogenic scoliosis is evident in a 16-year-old girl with a herniated disk at L4 to L5. A, the left scapula is high riding and hypoplastic, and its vertebral border is prominent. Knowledge of the normal anatomy and actions of the shoulder, arm, elbow, forearm, wrist, and hand is vital for assessment of abnormalities and institution of appropriate treatment. Sprengel Deformity A Sprengel deformity is a congenital malformation characterized by an abnormally small, high-riding scapula. The etiology is unknown, but there appears to be a familial predisposition, and the condition may be associated with a variety of other congenital anomalies, including Klippel-Feil syndrome. Cosmetic deformity and limited shoulder motion on the affected side are the usual complaints. On examination, the scapula is noted to be hypoplastic and high riding in association with asymmetry of the base of the neck and shoulders. This is due to limited scapular motion, because the scapula is often tethered to the cervical spine by a fibrous omovertebral band, which is frequently ossified. Nonsurgical treatment consisting of stretching and range-ofmotion exercises may be instituted but is rarely successful. Surgery may be undertaken on occasion for cosmetic and functional reasons and may consist of excision of the prominent superior aspect of the scapula or of release and reduction of the scapula accomplished by positioning it inferiorly on the chest wall. Although care must be taken during the procedure to prevent brachial plexus injury, surgery performed before adolescence usually improves appearance and restores some function. It is thought to result from a failure of maturation of the ossification center of the clavicle. It generally involves the right side and on occasion may be associated with other congenital anomalies and can be seen in patients with neurofibromatosis 1. In cleidocranial dysostosis, the entire clavicle may be absent or may have an appearance similar to that of congenital pseudarthrosis. On examination, the clavicle appears foreshortened with a prominence evident in its midportion. This condition characteristically involves no functional impairment and requires no treatment. Although clavicular fracture as a result of birth trauma may present a similar appearance, it is easily distinguished because of tenderness over the region of deformity. Radial Club Hand Radial club hand is the result of congenital absence or hypoplasia of the radial structures of the forearm and hand. A, the forearm is shortened with radial deviation of the hand and wrist on the ulna. B, A flexion deformity of the hand and wrist on the forearm and a hypoplastic thumb are present.
Toradol Dosage and Price
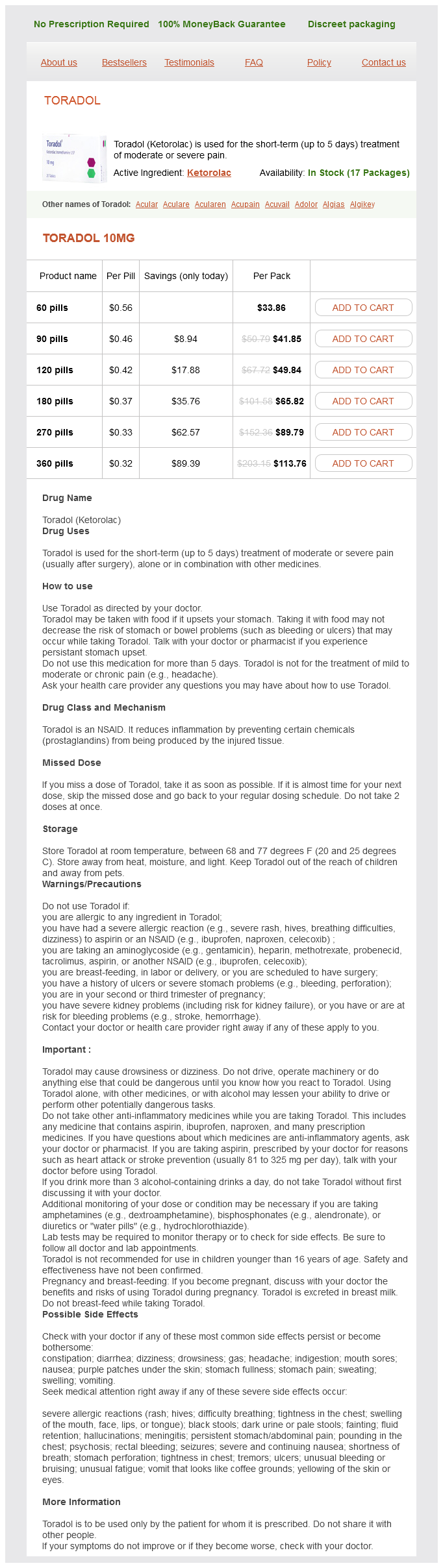
Toradol 10mg
- 60 pills - $33.86
- 90 pills - $41.85
- 120 pills - $49.84
- 180 pills - $65.82
- 270 pills - $89.79
- 360 pills - $113.76
Bacterial pathogens are isolated in 65% to 75% of patients from synovial fluid pain management from shingles buy toradol, blood, or both. The relative frequency of pathogens varies considerably with patient age, as shown in Table 13. Children with sickle hemoglobinopathies occasionally suffer Salmonella septic arthritis, whereas patients with Lyme arthritis may mimic a septic joint, but lack the severe outcomes. Neisseria gonorrhoeae is the organism most commonly associated with polyarticular disease, but other pathogens may be responsible, particularly S. Hip and shoulder joints are particularly prone to damage, because clinical signs may be subtle and thus diagnosis is delayed. Further, because the synovium inserts distal to the epiphysis of the proximal humerus and femur, compromise of the blood supply to the epiphysis is more likely to occur from increased intraarticular pressure. The classic picture of hematogenous septic arthritis is a young child with fever and signs of toxicity in association with severe localized joint pain, overlying swelling, and marked limitation in range of motion. Infants and toddlers cannot describe focal pain and thus present with fever and irritability, the latter aggravated by movement. Refusal to bear weight or decreased use of an extremity may have been noted by the family. When a knee, ankle, wrist, or elbow is involved, local swelling and warmth are usually evident. Erythema and warmth with septic arthritis are in contrast to what is often seen with Lyme arthritis. However, early swelling may be subtle, high fever may make any warmth difficult to distinguish, and surface erythema is often absent. When the hip is involved, swelling and warmth are not evident and pain may be referred to the knee or thigh. Examination of joint fluid revealed gram-positive cocci in chains, with a white blood cell count of 24,000/mm3. In cases of septic arthritis of the shoulder, subtle swelling may or may not be evident, but the shoulders may not be held at the same level and the arm on the involved side is held against the chest to splint the joint. Septic arthritis of the sacroiliac joint, which accounts for only 1% of cases, can present a particularly confusing picture, often mimicking hip or intraabdominal disease. Only one-third of patients have an acute presentation, the remainder having a subacute course. Findings of lower abdominal and rectal tenderness in association with normal hip motion may confuse the examiner who fails to recognize that leg and buttock pain necessitate meticulous examination of the lower back. Such an examination reveals tenderness over the involved sacroiliac joint, and pelvic compression replicates the pain, as does hyperextension of the ipsilateral hip with the patient supine and dangling his or her leg over the edge of the table. Limitation of joint motion and evidence of pain on motion are perhaps the most valuable clinical clues to the diagnosis of septic arthritis. Limitation is usually severe unless presentation occurs early, and motion provokes marked discomfort. Because of the morbidity associated with delayed diagnosis, any child with fever, acute onset of pain, and limited motion of a joint should be presumed to have septic arthritis until proven otherwise. Plain radiographs with comparison views should be obtained immediately and inspected for signs of joint space widening or capsular distention, although these findings may be absent in early cases. If the hip is the suspected site of pathology, lateral and upward displacement of the femoral head may be noted along with displacement of the gluteal fat lines. Arthrocentesis and examination of joint fluid is the study most likely to yield definitive results. Positive findings on Gram-stained specimens are particularly helpful; cultures are positive in 60% of cases. Elevated synovial white blood cell count of more than 50,000/ mm3 is present in more than two-thirds of patients. However, there is considerable overlap of cell counts in bacterial arthritis, rheumatologic syndromes, and Lyme arthritis. Thus, cell differential, protein, and glucose levels of synovial fluid are crucial. Up to 20% of patients have white blood cell counts less than 10,000/mm3, although most have a significant leftward shift. The sedimentation rate may be markedly elevated, but is less than 40 mm/hour in half of patients. Although radiographs may be normal early on, joint space widening can be detected. Plain film shows capsular swelling and lateral displacement of the proximal left femur. Diagnosis depends on assessment of clinical course, physical findings, and multiple laboratory studies. Even with negative Gram stain, empiric antimicrobial therapy selected to cover the most likely pathogens (see Table 13. As is true of osteomyelitis, collaboration between pediatric and orthopedic colleagues is crucial because drainage of infected material and joint irrigation are essential to ensure a good outcome. Any disorder associated with acute arthritis must be considered as part of the differential diagnosis of septic arthritis. In some instances, an obvious viral or vasculitic syndrome enables differentiation. The polymigratory picture of acute rheumatic fever and the much less acute onset of juvenile idiopathic arthritis help to distinguish these conditions. Adenopathy, visceromegaly, anemia, and radiographic changes help distinguish malignant joint infiltration. The highest risk population in the United States is foreign-born persons, especially from Mexico, the Philippines, India, Vietnam, and China. Among American-born persons, rates are highest among Native American, black non-Hispanic, and Hispanic populations.