General Information about Trimox
Trimox is mostly well-tolerated by patients, though some could expertise gentle side effects similar to nausea, diarrhea, and stomach upset. These unwanted side effects are normally momentary and subside as the physique adjusts to the treatment.
One of the most typical makes use of of Trimox is for treating ear infections. These are often attributable to micro organism within the center ear, which may result in ache, irritation, and even momentary hearing loss. Trimox helps to clear up the infection, relieving symptoms and stopping additional problems.
Another frequent use of Trimox is for the treatment of gonorrhea, a sexually transmitted an infection (STI) brought on by the micro organism Neisseria gonorrhoeae. Gonorrhea can cause extreme signs including painful urination, discharge, and in some circumstances, infertility. Trimox is a generally used antibiotic for treating this an infection, and is commonly very efficient in clearing up the symptoms.
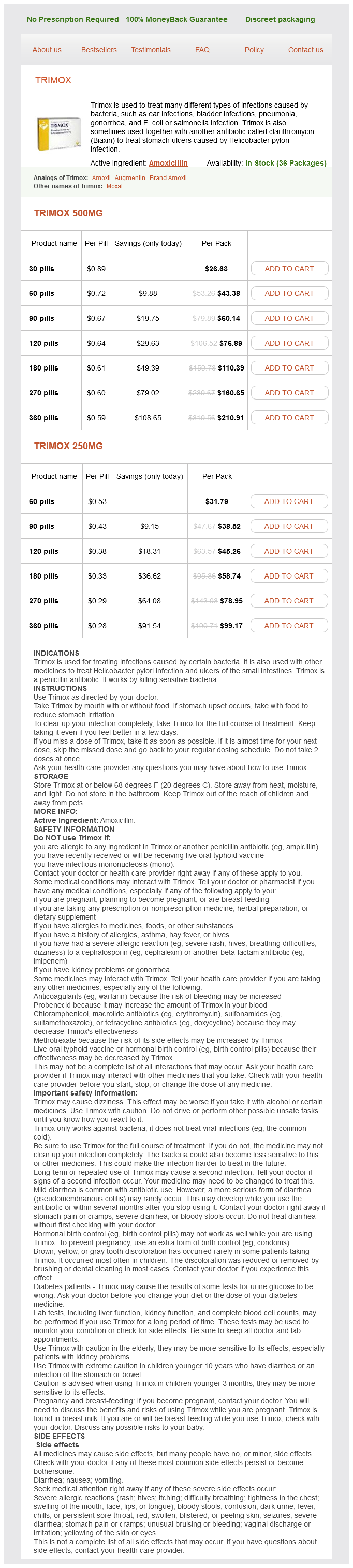
Trimox, also identified by its generic name amoxicillin, is a extensively used antibiotic that belongs to the penicillin family. It is used to deal with quite so much of infections attributable to micro organism, together with ear infections, bladder infections, pneumonia, gonorrhea, and sure types of stomach ulcers.
It is essential to note that whereas Trimox is efficient towards bacterial infections, it isn't effective towards viral infections such as the frequent chilly or flu. It can be important to finish the total course of the treatment, even if signs improve, to ensure that the an infection is totally eradicated and forestall the development of antibiotic-resistant micro organism.
The medication works by interfering with the growth of bacterial cell walls, thus stopping the micro organism from multiplying and inflicting further an infection. This makes it a extremely effective remedy for bacterial infections.
In addition to ear infections, Trimox can be prescribed for urinary tract infections (UTIs) such as bladder infection. UTIs are most commonly attributable to bacteria coming into the urinary tract, which may trigger painful urination, frequent urination, and a powerful urge to urinate. Trimox is an effective treatment for these varieties of infections, often providing aid inside a couple of days.
Trimox is also used to treat pneumonia, a severe infection of the lungs and respiratory system. Pneumonia could be attributable to a selection of micro organism, and may lead to signs similar to fever, coughing, and issue respiration. Trimox is often used in conjunction with other antibiotics to effectively treat pneumonia and stop it from worsening.
In abstract, Trimox is a commonly prescribed antibiotic that's used to deal with quite lots of bacterial infections. It is very effective in relieving symptoms and stopping additional complications. If you are prescribed Trimox, you will need to observe your healthcare provider's instructions and complete the total course of treatment to ensure a profitable recovery.
In addition to the above mentioned makes use of, Trimox can be generally prescribed in combination with one other antibiotic known as clarithromycin to treat stomach ulcers brought on by the bacteria Helicobacter pylori. These ulcers could be painful and can lead to serious problems, so you will want to deal with them promptly. The combination of Trimox and clarithromycin helps to get rid of the bacteria and promote healing of the ulcer.
Malignant transformation of somatic teratomatous tissues occurs in patients toward the older end of the age spectrum and in those with large tumors antibiotics for sinus infection and ear infection trimox 500 mg buy overnight delivery. When containing sebaceous material and hair, the lesion is diffusely or partially echogenic with sound attenuation. They may exhibit differentiation from any of the three embryonic layers (ectoderm, mesoderm and endoderm). A minority of mature teratomas are composed exclusively of tissues derived from a single germ layer, and are termed "monodermal teratomas". Prime examples are the so-called "dermoid cyst" (exclusively composed of skin elements) and struma ovarii (discussed later in this chapter). The cyst contents are usually abundant and composed of sebaceous material and hair elements. In exceedingly rare instances, the tumor displays tissue organization highly reminiscent of a fetus with skin covering the tumor surface, appendages resembling limbs, and poorly formed cranial or other bone structures (so-called homunculus or fetiform teratoma). Cystic cavity containing abundant hair elements and pasty sebaceous material, as well as a discrete nodule of soft tan to yellow adipose tissue (Rokitansky protuberance). Epidermal cyst rupture with subsequent foreign bodytype giant cell reaction to hair elements is often observed, sometimes obscuring or replacing the cyst lining. Some tumors feature a prominent vascular proliferation in the form of glomeruloid structures or confluent vessels associated with the neural tissue. Melanosis peritonei consisting of pigment-laden histiocytes within the peritoneal stroma. Benign or malignant secondary neoplasia arising from mature tissue of the teratoma. Most patients with this complication are postmenopausal and present with a mass with radiologic features consistent with teratoma but featuring rapid growth or involvement of adjacent structures. B of obvious teratomatous elements, the distinction between these possibilities may not be possible on pathologic grounds alone. As teratomas can be bilateral, the opposite ovary requires examination and possible biopsy at the time of operation. They are usually homozygous for polymorphic genetic markers, although heterozygosity has been documented in up to 35% of cases. The cells lining the follicles are cuboidal and contain oxyphilic to clear cytoplasm. The follicles are filled with eosinophilic colloid and sometimes birefringent calcium oxalate crystals. A component of benign Brenner tumor or mucinous cystadenoma can be rarely encountered. There are no uniformly accepted criteria to determine malignancy in this context, and thus criteria used in the eutopic thyroid should be strictly applied. Well-formed thyroid follicles of varying sizes, containing colloid and with minimal stroma in between, are seen. The follicular architecture and intrafollicular colloid are usually obvious in struma ovarii, facilitating the diagnosis. Thorough sampling and careful examination of the cyst wall are important, as normal-sized follicles may be scant and compressed by the dominant cyst. Mucin stains and thyroglobulin immunohistochemistry can be considered to confirm the diagnosis. Stromal luteinization (left) can be observed, typically at the periphery of the lesion. A deposit of mature thyroid tissue in the omental adipose tissue is seen in a patient with struma ovarii. Struma ovarii behaves indolently, including those with strumosis and the majority of those with "malignant transformation" as per criteria used in thyroid neoplasia. For this reason, some believe that more stringent parameters for malignancy in struma ovarii must be developed. Factors associated with tumor recurrence include large tumor size, presence of adhesions or ascites, and a solid microscopic appearance. Carcinoid syndrome occurs in a third of patients (typically older women with tumors >7 cm) and includes diarrhea, flushing, cardiac murmurs, pedal edema and hypertension. If they are associated with a mature cystic teratoma, they typically form a solid nodule in the wall of the cyst. Carcinoids associated with carcinoid syndrome are often larger and predominantly solid. Even more unusual is finding carcinoid in isolation, which is by definition a form of monodermal teratoma. Primary ovarian carcinoids have been classified into five different categories: insular, trabecular, strumal, mucinous, and mixed types. All these types feature cytomorphology typical of neuroendocrine neoplasms elsewhere. The tumor cells have prominent eosinophilic cytoplasm and sometimes distinct argentaffin granules. The nuclei are round and uniform and have the typical "salt-and-pepper" chromatin appearance. The islands are closely packed and smaller toward the periphery of the lesion, compared to the larger islands toward the center of the tumor.
This patient had no reported contact with cats infection large intestine best purchase trimox, raising the possibility of donor-derived infection. Cat-scratch disease commonly occurs in immunocompetent children as a self-limited febrile illness characterized by a cutaneous papule at the site of a cat scratch and accompanied by regional lymphadenopathy. Systemic symptoms are mild in immunocompetent hosts, whereas transplant recipients can present with fever, fatigue, myalgias, joint pain, and night sweats. Children often present with prolonged fever, abdominal pain, joint pain, headache, weight loss, and chills. Immunocompromised patients may have splenic or hepatic enlargement or both, and abdominal imaging usually identifies hypodense lesions in either or both organs. Recurrence has been reported, with one case of recurrent cat-scratch lymphadenitis described in a pediatric kidney transplant recipient. The indirect immunofluorescent antibody assay for detection of serum antibodies to antigens of Bartonella species is available at many commercial laboratories and through the Centers for Disease Control and Prevention. Immunofluorescent antibody IgG titer greater than 1:256 is consistent with acute infection, although lower titers (. Documentation of a fourfold increase in IgG titers can also be suggestive of recent infection. Warthin-Starry or Steiner silver stain demonstrates aggregates of small coccobacilli. There is often a mixed inflammatory infiltrate of both lymphocytes and neutrophils. Lesions often demonstrate dilated capillaries and cystic bloodfilled spaces scattered throughout the hepatic or splenic parenchyma. Identification of Bartonella in cultures is difficult due to its fastidious growth and culture techniques that are not sensitive. Culturing of Bartonella can require 1 to 4 weeks of incubation on blood agar plates under specific conditions. If culture is performed, specialized laboratories with experience in isolating Bartonella organisms are recommended for processing of cultures. Liver and spleen lesions, lymphadenopathy, and hepatomegaly have also been reported. Treatment of the underlying cause is prudent, but patients may also require corticosteroid therapy. They should be educated about obtaining and caring for pets, particularly cats and kittens. All pets should be seen regularly by a veterinarian and before introduction of the pet into the home. New pets should not be introduced during times of heightened immunosuppression (immediate posttransplant period or during treatment for rejection). Immunocompromised hosts should avoid all contact with cats younger than 1 year, stray cats, cats with fleas, or cats that bite or scratch. Although declawing of cats is not routinely recommended, patients should not engage in behavior that would cause a scratch or bite. If a scratch or bite should occur, it should be cleaned immediately and thoroughly. Testing cats for Bartonella infection is not recommended because cats can be transiently bacteremic. Good hand hygiene is always encouraged, especially after petting or caring for cats or kittens. Diagnosis the differential diagnosis of cat scratch disease includes other causes of lymphadenopathy and systemic symptoms in transplant recipients: cytomegalovirus, Epstein-Barr virus, and posttransplant lymphoproliferative disease, lymphoma, fungal or mycobacterial infections, and pyogenic abscesses. Unlike in immunocompetent hosts, response to treatment is usually prompt in the immunocompromised patient. Pediatric transplant recipients with granulomatous or suppurative disease, including hepatosplenic lesions, have been successfully treated with single agents or combinations of agents: aminoglycosides (gentamicin, amikacin), macrolides (azithromycin, erythromycin), tetracyclines (doxycycline), fluoroquinolones (ciprofloxacin), and trimethoprimsulfamethoxazole. In most cases, therapy was discontinued when all lymphadenopathy and/or hepatosplenic lesions had resolved. Shorter therapy has been associated with at least one reported recurrence of lymphadenitis in a pediatric kidney transplant recipient. It is important to note, however, that children younger than 8 years in whom a macrolide may be given, doxycycline is not recommended for more than 21 days. Macrolides can increase the serum concentration of some calcineurin inhibitors like tacrolimus, and rifampin is a potent hepatic enzyme inducer and interacts with many drugs. In addition to antimicrobial therapy, a decrease in immunosuppression is recommended if possible. Risk factors for disease fall into two broad categories: those that increase exposure to contaminated water sources (well water and water in large buildings such as hotels or hospitals) and those with impaired pulmonary or immune defense mechanisms, especially transplant recipients, children with hematologic malignancies, and those who use glucocorticoids. There have been no reports of transmission between patients and health care providers or between patients and other patients, although there has been one report of possible transmission between a son and his mother who cared for him in a nonventilated residential room for several hours. Children tend to have fever, which may be the only initial symptom, but respiratory symptoms eventually become more prominent. Cough is the most frequent symptom and can be accompanied by dyspnea, tachypnea, and pleuritic chest pain. Legionellosis in immunosuppressed patients may rapidly progress to respiratory failure. Chills, abdominal pain, nausea and vomiting, headache, malaise, anorexia, and/or fatigue may occur. Diarrhea is a common extrapulmonary finding in adults but is infrequently reported in children. Extrapulmonary manifestations rarely occur in children, including Legionella-associated transverse myelitis and liver abscesses.
Trimox Dosage and Price
Trimox 500mg
- 30 pills - $26.63
- 60 pills - $43.38
- 90 pills - $60.14
- 120 pills - $76.89
- 180 pills - $110.39
- 270 pills - $160.65
- 360 pills - $210.91
Trimox 250mg
- 60 pills - $31.79
- 90 pills - $38.52
- 120 pills - $45.26
- 180 pills - $58.74
- 270 pills - $78.95
- 360 pills - $99.17
The diagnostic criteria for this malignancy in the context of endometriosis are the same as in the eutopic endometrium antibiotic xy order trimox 250 mg without prescription. Conservative therapy with analgesics can be considered in patients with limited disease. In severe cases or in patients with mass-forming endometriosis, laser ablation and/or surgical excision may be necessary. In patients with symptomatic uncomplicated endometriomas, simple cystectomy is indicated. Not infrequently, these specimens are sent for intraoperative analysis to exclude the presence of a secondary malignancy, which would indicate the need for a more comprehensive surgery. As patients with endometriosis have multifocal disease, they are at risk for malignant transformation at other sites. The biologic significance of atypical endometriosis is still not fully elucidated. It is, however, regarded as a indolent form of endometriosis since it lacks definitive molecular and clinical features of malignancy. Oophoritis secondary to viral, fungal, or parasitic infection is rarely encountered. Most women with infectious oophoritis present with symptoms of pelvic inflammatory disease, including pain, fever and/or vaginal discharge. Chronic pelvic inflammatory disease may be insidious in onset and recognized only when scarring of the fallopian tube and ovarian surface is identified during investigation for infertility. Although oophoritis is more commonly associated with ascending infections, it may also occur after fistula formation from the gastrointestinal tract (in the setting of diverticulitis, appendicitis or Crohn disease). Autoimmune oophoritis results in premature ovarian failure with early onset of menopause, usually preceded by a variable period of oligomenorrhea; there may be other autoimmune manifestations such as Hashimoto thyroiditis, Graves disease, or Addison disease. The infiltrate is typically most severe in the theca layers and becomes more intense with progressive maturation of the follicle. The main histologic differential diagnosis includes endometriosis; however, the presence of endometrial-type stroma and glands and the lack of a prominent inflammatory infiltrate are distinguishing features. In end-stage cases of autoimmune oophoritis or in small biopsies, the findings may be equivocal and correlation with clinical findings is necessary for diagnosis. A prominent lymphoplasmacytic infiltrate associated with fibrosis is present within the wall of a follicle. If chronic, secondary sequelae include extensive scarring and adhesions, obliteration of the fimbria, dilation of the fallopian tube (hydrosalpinx) and adherence to the ovary. Although there are no specific gross findings associated with autoimmune oophoritis, patients may have bilateral ovarian enlargement with multiple follicle cysts. This is rarely done on pathologic examination alone, unless fungi, mycobacteria or typical Actinomyces colonies are found histologically. Surgery is not indicated in most patients but will occasionally be required if there is abscess rupture, poor response to antibiotic therapy, or severe chronic pelvic pain and/or obstruction due to adhesions. The frequency of infertility after medical treatment of tubo-ovarian abscess is high and related to chronic scarring of the fallopian tube and ovary. An unusual complication of surgery for tubo-ovarian abscess is the ovarian remnant syndrome, in which scant ovarian tissue is left in the pelvic sidewall presumably because of ovarian surface adhesions. Although immunosuppressive therapy can be used empirically, it has shown inconsistent results. Striking acute inflammation with abscess formation and edema is typical of the acute phase of tubo-ovarian abscess. Rarely, granulomas may be present, and in such cases, tuberculosis, fungal and parasitic infections should be excluded. Granulomas may also be secondary to foreign body (foreign material or keratin), electrocautery or systemic disease (sarcoid, Crohn disease, giant cell arteritis). Healing and chronic phases of infectious oophoritis reveal extensive fibrosis and adhesions, typically obliterating the normal anatomy. Histopathology of ipsilateral and contralateral ovaries and plasma interleukin 6 levels after unilateral ovarian torsion. Fibromatosis and massive edema of the ovary, possibly related entities: a report of 14 cases of fibromatosis and 11 cases of massive edema. Two types of ovarian cortical inclusion cysts: proposed origin and possible role in ovarian serous carcinogenesis. Impact and mechanistic role of oral contraceptive pills on the number and epithelial type of ovarian cortical inclusion cysts; a clinicopathology and immunohistochemical study. European Journal of Obstetrics & Gynecology and Reproductive Biology, 209, 100104. The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects. Ovarian stromal hyperplasia and ovarian vein steroid levels in relation to endometrioid endometrial cancer. A103: An anti-melan-A monoclonal antibody for the detection of malignant melanoma in paraffin-embedded tissue. Clinicopathologic study of 19 cases with immunohistochemical analysis of steroidogenic enzymes. Pregnancy luteoma: A study of 20 cases on the occasion of the 50th anniversary of its description by Dr.