General Information about Verapamil
Verapamil belongs to a category of medicines known as calcium channel blockers. It works by blocking the entry of calcium ions into the muscles of the guts, which relaxes and widens the blood vessels, permitting for improved blood circulate and a slower coronary heart rate. This helps to lower the workload and oxygen demand of the guts, making it particularly helpful in treating SVT.
Verapamil is a broadly prescribed and generally protected medicine that has been used for many years in the treatment of SVT. However, you will need to note that it is probably not suitable for everybody. Patients with certain coronary heart circumstances, liver or kidney disease, or a historical past of heart failure ought to consult with their physician before taking this medication. Additionally, pregnant or breastfeeding women ought to search medical recommendation earlier than starting Verapamil remedy.
In conclusion, Verapamil is a commonly used medication for the treatment of supraventricular tachycardia. By blocking calcium channels within the heart, it helps to regulate the guts price and improve symptoms of SVT. While it is generally well-tolerated, precautions should be taken, and patients ought to intently monitor for any potential unwanted effects. With proper medical guidance, Verapamil can provide important reduction for those dwelling with SVT, allowing them to guide a more regular and cozy life.
As with any medicine, there are some potential unwanted side effects related to Verapamil. These can embrace dizziness, headache, flushing, low blood stress, constipation, and nausea. In uncommon instances, extra severe unwanted effects might occur, corresponding to irregular heartbeat, heart failure, or allergic reactions.
It is necessary to comply with the dosage instructions carefully and to observe for any adverse effects. Patients should also inform their physician of another medicines they're taking, as Verapamil could interact with sure antibiotics, blood thinners, and different medications.
Verapamil, additionally identified by its brand name Calan, is a extensively used treatment for treating supraventricular tachycardia (SVT). SVT is a kind of coronary heart rhythm dysfunction the place the guts beats faster than normal, typically above a hundred beats per minute. It is brought on by irregular electrical impulses in the higher chambers of the guts, often known as the atria.
When taken as directed, Verapamil can successfully control the symptoms of SVT, including heart palpitations, chest pain, and shortness of breath. It can even scale back the frequency and severity of SVT episodes and improve the overall high quality of life for these dwelling with this situation.
Verapamil is on the market in several forms, including immediate-release tablets, sustained-release tablets, and extended-release capsules. The dose and frequency of administration depend on the individual’s medical situation and response to the medicine. Often, the doctor will begin with a decrease dose and steadily improve it to attain the specified impact.
Speckle tracking relies on the automated tracking of unique acoustic backscatter during standard grayscale imaging prehypertension and anxiety discount verapamil 80 mg with mastercard. Both strain and its planar dimensions may be assessed using semiautomated off-line analysis, which improves reproducibility and feasibility. This technique is promising and is currently being used as a measure of mechanical dyssynchrony in ongoing clinical trials. Furthermore, the secondary end point of all-cause mortality reached statistical significance after 3 years of follow-up, and the survival curves continued to separate. The primary end point of all-cause mortality and hospitalization was significantly different in the device groups as compared with the medically treated group. The trial was not powered to compare mortality benefits between the two device groups. Their symptoms do not improve or worsen, and there is no echocardiographic evidence of reverse ventricular remodeling. Areas of fibrous myocardium are electrically and mechanically nonviable; therefore, pacing at those sites may be of little value. Based on the inclusion criteria from the available large randomized trials at that time (see Table 56. All patients receive preprocedural antibiotics at least 30 minutes before the procedure. If high pacing threshold or diaphragm capture occurs, the lead should be repositioned. Because the pressure in the venous system is low, serious sequelae are unusual and cardiac tamponade rarely results. For that same reason, patients are encouraged to ambulate while still in-house to prevent any out-of-hospital dislodgement, which may have more serious consequences. Given the two ventricular inputs (right ventricle and left ventricle), one could foresee that ventricular timing cycles could be quite complex during Bi-V pacing. While such clinics are limited mostly to specialized centers, such clinics have been shown to convert some nonresponders to responders. Any evidence of lead malfunction or displacement should be dealt with promptly by reintervention. Patient selection and echocardiographic assessment of dyssynchrony in cardiac resynchronization therapy. Developed with the special contribution of the Heart Failure Association and the European Heart Rhythm Association. There is an rsR pattern in leads V1 and V2, representing delayed activation of the right ventricle. Temporary pacing is indicated in patients with acute hemodynamically significant bradycardia or asystole. Reversible causes such as digitalis toxicity, antiarrhythmic agents, and electrolyte disturbances such as hyperkalemia should be determined and reversed. Temporary pacing is indicated for overdrive pacing and termination of atrial flutter (type I with long excitable gap) or supraventricular tachycardia due to a reentrant mechanism. Temporary pacing may be used as a bridge to permanent pacing in patients with complete heart block, high-grade second-degree block, severe sinus node dysfunction, and asystole. Generally, temporary pacing in this setting is for patients with an acute illness (endocarditis and systemic infection elsewhere) that delays permanent pacemaker placement. Monomorphic ventricular tachycardia can be terminated with antitachycardia pacing through a ventricular temporary wire by pacing at a rate faster than the tachycardia. Overdrive pacing is initiated at 10 to 15 beats per minute (bpm) faster than the tachycardia. Pacing is done for several captured beats (up to 10 to 15 seconds) and then abruptly stopped. If tachycardia persists, the pacing rate is sequentially increased by 10 bpm and pacing repeated. The major potential complication of this technique is conversion to a faster or unstable rhythm. The advantage is that post-tachycardia pauses can be managed with pacing if necessary, and direct current cardioversion may be avoided. In certain forms of myocarditis with heart block, such as Lyme disease, or post cardiac surgery, temporary pacing can be used because there is a significant chance of recovery of conduction. Pacing to increase heart rate in patients with acute aortic regurgitation who have bradycardia and elevated left ventricular end-diastolic pressure can reduce diastolic filling time and improve hemodynamics. Patients who are undergoing alcohol septal ablation for hypertrophic cardiomyopathy receive prophylactic transvenous pacers, given the significant risk of complete heart block during the procedure. Patients who are undergoing balloon aortic valvuloplasty and percutaneous aortic valve replacement have a temporary pacemaker placed for overdrive pacing during balloon inflation and valve implantation. Temporary atrial, coronary sinus, and ventricular pacemakers are frequently used for electrophysiologic studies. Transcutaneous ventricular pacing involves placement of large-surface-area, high-impedance electrodes (Zoll pads) on the anterior (over lead V3 or the palpable cardiac apex) and posterior chest walls (inferior aspect of the scapula, to the left or right of the spine). It usually requires long pulse widths (20 to 40 milliseconds) and high outputs of up to 100 to 200 mA. Transcutaneous pacing may be useful when transvenous pacing is contraindicated and in code situations. It avoids the complications associated with transvenous pacers such as pneumothorax, right ventricular perforation, infection, bleeding, and venous thrombosis.
Sirolimus (rapamycin) halts and reverses progression of allograft vascular disease in non-human primates hypertension obesity buy generic verapamil line. Revision of the 1990 working formulation for the standardization of nomenclature in the diagnosis of heart rejection. Molecular testing in the management of cardiac transplant recipients: initial clinical experience. Cardiovascular magnetic resonance in the diagnosis of acute heart transplant rejection: a review. Detection and prediction of acute heart transplant rejection with the myocardial T2 determination provided by blackblood magnetic resonance imaging sequence. International Society for Heart and Lung Transplantation working formulation of a standardized nomenclature for cardiac allograft vasculopathy 2010. Scientific registry of solid-organ transplant recipients in the United States ( It is essential for the specialist as well as the internist to have a high index of clinical suspicion for this devastating disease, as early diagnosis and referral may affect the survival. Data from registries estimate the prevalence at around 15 to 50 cases/million adults and its incidence at around 2. Most commonly, it occurs with conditions where blood flow is high and the pulmonary vasculature is exposed to systemic level pressures. These symptoms may include dyspnea on exertion, fatigue, weakness, chest pain, palpitations, syncope, abdominal distention, and pedal edema. Findings of telangiectasia, digital ulceration, and sclerodactyly suggest scleroderma, while inspiratory crackles may point toward interstitial lung disease. Patients should be carefully screened for the presence of stigmata of liver disease, such as spider naevi, testicular atrophy, and palmar erythema. The presence of clubbing suggests congenital heart disease or pulmonary veno-occlusive disease. In patients with systemic lupus erythematosus, anticardiolipin antibodies may be found. In advanced stages of the disease, atrial flutter or atrial fibrillation often occurs, leading to further clinical deterioration. The chest x-ray may also point to lung abnormalities and show features suggestive of left heart disease. By using the Doppler technique, peak velocity of the tricuspid regurgitation jet can be measured. From this measured velocity, the pressure difference between right ventricle and right atrium can be estimated by employing the simplified Bernoulli equation (P = 4v2). Cardiac output can be determined using the thermodilution method and/ or the Fick method (measurement of mixed venous saturation SvO2 needed). This decrease may give a false impression of hemodynamic improvement or suggest that there is mild to moderate disease. Pharmacological impact on right ventricular remodelling in pulmonary arterial hypertension. In veno-occlusive disease and left heart disease, it can even provoke pulmonary edema. If clinically suspected, screening overnight polysomnography may diagnose significant obstructive sleep apnea. In addition to the distance walked, the degree of dyspnea (Borg score) and oxygen saturation are also measured. A 6-minute walk distance of < 332 m and a drop in oxygen saturation by > 10% are suggestive of poor prognosis. It is also measured on routine follow-ups and can be indicative of clinical deterioration. These low-pressure, low-resistance, and high-compliance characteristics of the pulmonary vascular bed are regulated by a balance between vasodilators and vasoconstrictors and between cell proliferation and apoptosis. Genetic and environmental factors may disturb this balance, resulting in excessive vasoconstriction, vascular remodeling, and micro-thrombosis, which leads to pulmonary (arterial) hypertension. Our understanding of these factors and various pathologic forces is limited, but some pathways have been elucidated mainly due to their therapeutic potential. Prostacyclin/thromboxane A2: Prostacyclin and thromboxane A2 are arachidonic acid metabolites in vascular cells. Prostacyclin has potent vasodilating, antiproliferative, and platelet-inhibiting properties, whereas thromboxane A2 has the opposite effect. It is a potent vasodilator and an inhibitor of platelet activation and of vascular smooth muscle cell proliferation. Prostacyclin analogs: Prostacyclin is a potent endogenous vasodilator and an inhibitor of platelet aggregation and also appears to have antiproliferative activity. Adverse events related to the delivery system include pump malfunction, local site infection, catheter obstruction, and sepsis. Sildenafil (Revatio) has favorable effects on exercise capacity, symptoms, and hemodynamics. Combination therapy is being routinely employed if treatment goals are not achieved with one compound ("goal-directed therapy"). There is some evidence of improvement in the quality of life, exercise performance, and hemodynamics with sildenafil in patients with left heart disease and in patients bridged to transplantation with a left ventricular assist device. It is recommended that surgical evaluation and procedure be performed at high volume centers. This may help target future research and identify these patients who would benefit from management at a specialized center where a multidisciplinary approach may be provided. Evaluating disease severity and predicting survival is important because it may guide clinical management. There is registry level evidence that prognosis has improved with pulmonary vasodilator therapies.
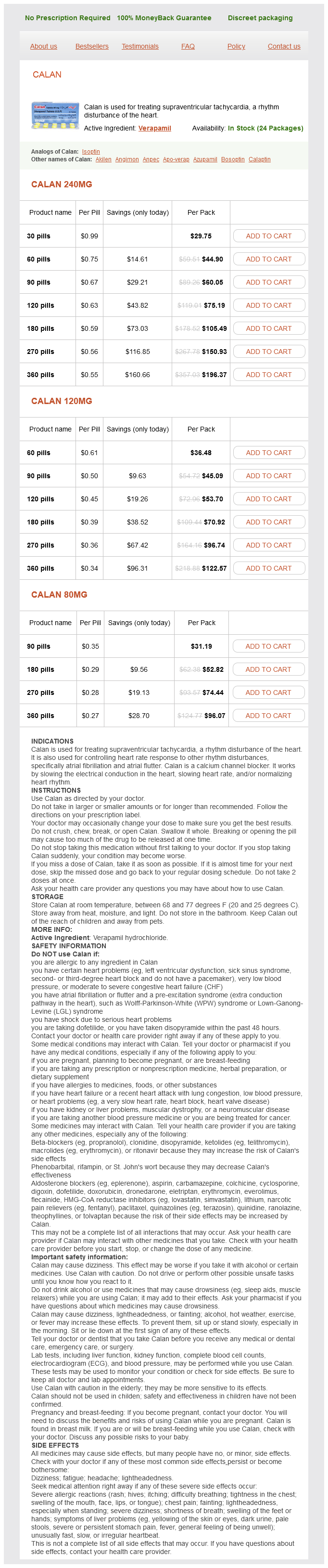
Verapamil Dosage and Price
Calan 240mg
- 30 pills - $29.75
- 60 pills - $44.90
- 90 pills - $60.05
- 120 pills - $75.19
- 180 pills - $105.49
- 270 pills - $150.93
- 360 pills - $196.37
Calan 120mg
- 60 pills - $36.48
- 90 pills - $45.09
- 120 pills - $53.70
- 180 pills - $70.92
- 270 pills - $96.74
- 360 pills - $122.57
Calan 80mg
- 90 pills - $31.19
- 180 pills - $52.82
- 270 pills - $74.44
- 360 pills - $96.07
It affects both ventricles (50%) blood pressure value chart 120 mg verapamil order mastercard, left ventricle (40%), or isolated right (10%) ventricle and is associated with a 2-year mortality rate of up to 50%. This technique has high operative mortality (15% to 20%), but when successful, reduces symptoms and may favorably affect the survival. Features include eosinophilia, restrictive cardiomyopathy, and nervous system and marrow involvement. It usually occurs sporadically, but may be inherited with an autosomal dominant pattern in association with distal skeletal myopathy and occasionally a heart block. Cardiac sarcoidosis can present with restrictive cardiomyopathy, but much more commonly it produces a dilated cardiomyopathy phenotype. Associated cardiac manifestations include conduction disease and ventricular tachyarrhythmia. Direct myocardial involvement, usually in the form of diastolic dysfunction, can be underappreciated, particularly when there is concomitant valvular, coronary, and/or pericardial disease. Separating the relative contributions of multiple pathophysiologic mechanisms in a given radiation patient is extraordinarily challenging. Metabolic storage diseases are characterized by intracellular deposition of substances within the myocyte, resulting in increased myocardial stiffness. Hemochromatosis, or iron overload, is listed as a storage disorder that can cause restrictive cardiomyopathy. However, when cardiac manifestations occur, the phenotype is usually a dilated cardiomyopathy. This leads to glycosphingolipid accumulation in the kidney, the skin, and the heart. Echocardiography is the primary modality in evaluating a patient with a clinical syndrome of congestive heart failure. There are numerous other 2D and Doppler findings that are critical to diagnosis, including chamber size and wall thickness. The atrial kick is proportionately greater, and EA reversal occurs, with an E/A ratio < 1 (grade 1 diastolic dysfunction). When the deceleration time is < 160 milliseconds and the E/A ratio is > 2, the patient is considered to have grade 3 diastolic dysfunction. Although the transmitral flow pattern is one of the primary ways of evaluating diastolic function, it has several limitations. In the earliest stages of diastolic dysfunction, the diastolic velocities of annular motion decrease. This correlation is better with patients with depressed ejection fraction but is reasonable in patients with normal ejection fraction. For these patients, the presence of elevated filling pressure cannot be determined by this method alone. In patients with predominantly exertional symptoms, it may be useful to perform exercise echocardiography to determine the presence of diastolic dysfunction during exertion, particularly when this is not evident at rest. Invasive hemodynamic assessment is not routinely performed but is indicated when it is unclear whether elevated filling pressures are present on noninvasive studies. Other diastolic parameters, including Tau, the time constant of isovolumic relaxation, are rarely measured in clinical practice. When restrictive cardiomyopathy is considered, detailed hemodynamics may be of greatest value in directing management but are often less helpful in differentiating between possible diagnoses. It is useful to measure ventricular function, mass, and volumes when echocardiography is not diagnostic. It is also helpful in establishing or excluding specific conditions such as constrictive pericarditis, sarcoidosis, amyloidosis, or hemachromatosis (see Chapter 51). Biopsy in this setting can determine the presence of amyloid as well as differentiate between the different types of amyloid. Patients should be placed on a salt-restricted diet, usually 2,000 mg of sodium daily. For this indication, hydrochlorothiazide (usually 50 mg dosage, given once or intermittently) is effective within the first day. In extreme cases, patients may have significant bowel edema, rendering diuretics with poor oral absorption ineffective. In these patients, torsemide, which has a better oral absorption profile, is a reasonable option. On occasion, the patient may only achieve symptomatic relief after aggressive diuresis, even to the point where the blood urea nitrogen and/or creatinine are at levels higher than baseline values. This trial showed no difference in the primary end point of mortality and heart failure hospitalizations between the active and placebo groups. The primary end point was not met, but after 1 year, there appeared to be a statistically significant decrease in heart failure hospitalizations in the active treatment arm. In the overall trial, the nebivolol group demonstrated a significant decrease in the primary end point of mortality and heart failure mortality. There was a nonsignificant trend toward decreased heart failure hospitalizations but an increased trend toward unstable angina hospitalizations in those treated with digoxin. In patients with depressed ejection fraction, aldosterone antagonists have been demonstrated to have beneficial effects, likely working through antifibrotic mechanisms. Even in the presence of this diagnosis, specific treatment or change in management is uncertain.