General Information about Zofran
In conclusion, Zofran is a extremely efficient treatment used to forestall nausea and vomiting in patients undergoing cancer therapy or surgical procedure. It works by focusing on serotonin receptors in the physique, lowering the nerve indicators that set off these symptoms. While it might trigger some side effects in some individuals, the advantages of this treatment outweigh the potential risks, making it an invaluable software within the administration of nausea and vomiting. If you're experiencing these symptoms as a outcome of chemotherapy or surgery, discuss to your physician about whether Zofran is an appropriate option for you.
There are various types of Zofran out there, together with tablets, oral disintegrating tablets, and injectable solutions. The dosage and methodology of administration will depend on the patient's medical situation and individual wants. It is important to take Zofran as directed by a healthcare skilled and comply with the prescribed dosage rigorously.
Zofran is a drugs generally used within the prevention of nausea and vomiting brought on by certain medical therapies, such as most cancers chemotherapy and surgery. It belongs to a category of medicine often identified as antiemetics, which work by blocking the actions of chemicals in the physique that may trigger nausea and vomiting. This treatment has been a game-changer for so much of sufferers undergoing most cancers therapy or surgery, because it helps to reduce the uncomfortable and unsightly unwanted effects of these procedures.
One of the main makes use of of Zofran is in most cancers sufferers who are receiving chemotherapy. Chemotherapy is a standard form of cancer therapy that includes utilizing powerful medicine to kill most cancers cells. While chemotherapy may be efficient in preventing cancer, it additionally comes with a range of unwanted effects, some of the vital being nausea and vomiting. These side effects may be debilitating and may have a significant impression on a affected person's quality of life. Zofran is often prescribed alongside chemotherapy to help forestall these signs and permit sufferers to continue their treatment with out interruption.
While Zofran is generally well-tolerated, like several treatment, it may cause unwanted side effects in some people. The most common unwanted side effects of Zofran embody headache, dizziness, constipation, and fatigue. These unwanted effects are usually gentle and momentary, and most sufferers don't expertise any important points while taking this treatment. However, it's essential to tell a healthcare provider if any extreme or persistent side effects happen.
In addition to its use in most cancers sufferers, Zofran is also helpful for patients who endure surgery. Surgery, no matter its type, is normally a tense experience for the physique, and it isn't unusual for patients to experience nausea and vomiting after recovering from anesthesia. Zofran could be administered before surgical procedure to help stop these signs from occurring, making the post-operative recovery course of more comfortable for the affected person.
Zofran works by blocking the actions of serotonin, a chemical in the physique that can set off emotions of nausea and vomiting. This medication targets serotonin receptors within the gut and the brain, serving to to scale back the nerve signals that cause nausea and vomiting. By doing so, Zofran successfully helps to prevent these symptoms, providing relief to patients undergoing chemotherapy or surgical procedure.
In rare instances, Zofran may cause a potentially serious side effect known as serotonin syndrome, which might happen when there is an excess quantity of serotonin within the body. Symptoms of serotonin syndrome embody confusion, agitation, muscle stiffness, fever, and irregular heartbeat. If any of those symptoms occur, it's essential to hunt medical consideration immediately.
Relative to small molecule transmitters symptoms dengue fever buy zofran 4 mg with visa, peptides have slower, longer-lasting effects. They can augment or reduce the effect of small molecule transmitters when they are released. Peptides can be present in the same terminal button as small molecule transmitters but are located in separate vesicles. Peptides differ from small molecules in a number of ways (Fairchild, 2011; Belzung et al. Once released, peptides are deactivated by enzymes and are not taken up by the terminal button and recycled. Peptides are released in larger amounts from various regions of the terminal button. Peptides diffuse throughout the extracellular fluid and are capable of modulating the activity of neurons in a wider region. Peptides can increase the sensitivity of postsynaptic receptors to small molecule transmitters. Small Molecule Transmitters the three classes of small molecule transmitters are amino acids, monoamines, and acetylcholine. Amino acids are the building blocks of proteins and are widely distributed throughout the brain. They contain both a carboxyl group and an amino group attached to the same carbon. The amino acids are the major transmitters in the brain, while the remaining neurotransmitters account for a relatively small percentage of synapses (Cooper et al. Aspartate Although abundant in the brain, relatively little is known about aspartate (aspartic acid). Both aspartate and glutamate serve as building blocks for proteins and peptide synthesis, and are involved in intracellular metabolism (Cooper et al. Aspartate typically produces an excitatory effect (depolarizes) on the membrane and is closely related to glutamate. Receptor dysfunction for both amino acids has been implicated in schizophrenia (Kim, Kaufman, et al. Glutamate Glutamate is the principal excitatory neurotransmitter in the brain, accounting for approximately 50% of synapses (Snyder & Ferris, 2000). Glutamatergic neurons are widely 66 Cellular Function, Neurotransmission distributed-in subcortical structures, throughout the cortex, and in other areas of the brain. Glutamate is biosynthesized in the cell via a series of enzymatic changes beginning with precursors. Ionotrophic as well as metabotrophic receptors specific to glutamate have been identified (Sheng, 2001; Petralia, Al-Hallaq, & Wenthold, 2009; Pittenger, 2015). These receptors consist of complex subunits that interact with intracellular proteins, but the specific functions of the subunits are not fully understood. Glutamate receptors are usually located on parts of the dendrite and less commonly near or on the cell body (see von Bohlen und Halbach & Dermietzel, 2002 for a review). Glutamate is cleared from the cleft primarily by glia cells (astrocytes) via transporter proteins found on the glial cell membrane. Glutamate is also reclaimed from the synaptic cleft by transporter proteins located on the presynaptic neuron (Albrecht & Zieliska, 2017; Cooper et al. After glutamate is cleared from the cleft by glial cells enzymes convert it into glutamine. Glutamine is then transported to neuronal terminal buttons, where it serves as a precursor for the biosynthesis glutamate. The reuptake process is particularly important, as high levels of extracellular glutamate can be toxic to other neurons and glia cells, as discussed in Chapter 1. For example, Michael and colleagues (2003) reported that adults suffering from bipolar disorder and mania had significantly elevated levels of glutamate in the region of the prefrontal cortex. Schiffer (2002) reviewed molecular genetics findings and concluded that mutations in glutamate receptor genes might increase the risk of developing schizophrenia, bipolar disorder, or depression. Levine and colleagues (2000) compared cerebral spinal fluid glutamate metabolites in adults with depression (unipolar and bipolar) relative to control subjects and found that those suffering from depression had higher metabolite concentrations. Glutamate has also been found to influence the release and inhibition of other neurotransmitters such as serotonin. Marek (2002), for example, reported that drugs that stimulate glutamate autoreceptors suppress the release of glutamate, which in turn reduces the release of serotonin in the prefrontal cortex. Recent research has focused on the role of glutamate and glutamate agonists in major depressive disorders (Abdallah et al. One of the difficulties in determining the role of glutamate or other neurotransmitters in pathological conditions is that the complexities of these neurotransmitters systems in the normal brain are not yet understood. Widely distributed throughout the brain, it is found in higher concentrations in the limbic system, basal ganglia, and cortex. Monoamine Neurotransmitters the monoamine neurotransmitters fall into two main groups: catecholamines and indolamines. Dopamine Dopamine cell bodies are heavily concentrated in the basal glanglia, substantia nigra, and tegmentum and have widespread projections to the frontal regions of the brain, and to a lesser extent, other regions of the brain. Each system is associated with specific functions, and the morphology and density of the neurons vary among the systems (Cooper et al. These disorders and the role of the dopaminerigic systems, as well as other neurotransmitter systems, are addressed in subsequent chapters. The pathway involved in the biosynthesis of dopamine was first proposed in 1939 by Blaschko (1939), and according to Meiser (2013), this process is highly complex, with many unanswered questions remaining. Five families of dopamine receptors have been identified, all of which are metabotropic receptors. According to Greengard (2001), the second-messenger pathways involved in these metabotropic receptors are enormously complicated.
Another important area of recent emphasis has been the double power of vaccinations for pregnant women medicine 3604 pill buy zofran 4 mg overnight delivery, protecting two-mother and infant-against the targeted pathogen. In addition, a critical need for prepregnancy vaccination to protect pregnant women and their fetuses ahead of and during the highly vulnerable first trimester of pregnancy is currently underscored by acquisition of Zika virus infections during pregnancy with resulting microcephaly and other birth and developmental anomalies. Community protection (also termed herd immunity) of seniors by vaccination of children, who are the primary spreaders of many vaccine-preventable infectious diseases, and younger adults can provide dramatic reductions in infectious disease incidence in seniors-for example, the reduction in pneumococcal disease in seniors after the introduction of pneumococcal conjugate vaccine for children. Vulnerable community members whose immune systems are unable to respond well to vaccines (newborns, immunocompromised persons, older adults) or are unable to receive vaccines (because of allergy or a medical contraindication) depend on immunization of surrounding community members for protection against vaccine preventable diseases. The vaccinated community becomes an immunological cocoon or wall of protection for these vulnerable members of society. This article first reviews selected events in the history of vaccination, both distant and recent. The remarkable accomplishments that have resulted from programs of vaccination to date are then highlighted. We also describe important recent milestones and changes in vaccine development strategies that have the potential to revolutionize the field and offer great hope for providing solutions for unmet vaccine needs. Finally several present and future challenges for the field of vaccinology are discussed. If the recipient survived, he or she was protected against future smallpox disease. Since natural smallpox had a 30% mortality rate and variolation had a lower (1%) mortality rate, this ancient practice was an early example of weighing the risk-to-benefit ratio for a human health intervention. By 1700, variolation was employed in a number of societies in Africa, India, and the Ottoman empire, and it was in use in England and France in the 1700s. In 1796, an English physician was searching for a safer alternative to variolation. He performed a smallpox vaccination experiment on James Phipps on May 14, 1796, using as vaccine cowpox pus from the lesions on the hands of Sarah Nelmes, a milkmaid. Other opponents of vaccination were those with financial interests in lucrative variolation practices. When vaccination in England was made compulsory by the Vaccination Act of 1853, an organized antivaccination movement arose almost immediately. The observation of the protected state (immunity) in dairymaids led to a concept that was tested and promoted by Jenner. This would not be permissible today in smallpox research, although human challenge experiments are performed for certain self-limiting or treatable infectious diseases. Young Phipps survived both the vaccination and the challenge, and Jenner first reported his experiment in 1797 in a short communication to the Royal Society. Access can be provided through referral or by stocking and administering the indicated vaccines. The postvaccination challenge experiment can be an important process to efficiently obtain preliminary protective efficacy information for a vaccine and has been shown in early-phase clinical trials to be safe, well tolerated, and immunogenic. Human challenge studies are performed for self-limiting and/or treatable infections to study vaccine protection or to characterize host response to infection in detail. A human challenge experiment can rapidly provide feedback to vaccine developers and public health officials to help prioritize resource-intensive field trial evaluations of promising candidate vaccines. This is particularly advantageous in the context of an epidemic, where rapid vaccine development and deployment are needed for optimal impact on morbidity and mortality. A contemporary example is Zika virus vaccine development-for which postvaccination human challenge experiments are under consideration. The miasma theory (which postulated that infectious diseases were caused by a noxious form of bad air) was gradually replaced by the development of the germ theory (according to which infectious diseases were caused by microorganisms too small to be seen without magnification). Animal experiments and laboratory cultivation of microbes were key advances relating to the germ theory in the second half of the nineteenth century. Robert Koch (18431910) and the great French chemist Louis Pasteur (18221895) made significant contributions through their many key observations and experiments in both agricultural and human infectious diseases and vaccines. Through attenuation or inactivation of wild-type microbes, Pasteur produced vaccines that induced protection against a number of diseases. He performed a number of classic vaccination and challenge experiments in farm animals; these experiments were designed to show that in experimental challenges, his altered (attenuated or inactivated) cultures of microbes could be delivered as vaccines that offered protection to susceptible animals and herds against organisms that could be devastating, including veterinary pathogens, such as chicken cholera and anthrax, and human pathogens, such as rabies. Certainly in the 1700s and earlier centuries, the variolators and the great Jenner knew they had created a protected condition in their patients through their intervention only if their patient survived that intervention. But they had no specific knowledge of the killed or attenuated microbe they were administering, of the virulent microbe they were protecting against, or of the immune system changes induced in the bodies of their patients (or even of the existence of the immune system). In the nineteenth century, Pasteur and Koch certainly knew that microbes were the cause of infectious diseases and that weakened forms of microbes (vaccines) could create a protected state after administration to livestock or humans. In the early twentieth century, passive immunization was developed as a therapy for infectious diseases. Early work by Emil von Bering (18541917) with small-animal serum therapy experiments led to the development of human serum therapies for passive immunization. In 1900, von Bering used horse sera from immune horses to cure and prevent diphtheria caused by Corynebacterium diphtheria. The very first Nobel Prize in Physiology or Medicine in 1901 was awarded to von Behring "for his work on serum therapy, especially its application against diphtheria, by which he has opened a new road in the domain of medical science and thereby placed in the hands of the physician a victorious weapon against illness and deaths. The Nobel Prize in Physiology or Medicine for 1908 was awarded to Ilya Ilyich Mechnikov (18451916) and Paul Ehrlich (18541915) "in recognition of their work on immunity" and for establishing the concepts of cell-mediated and humoral immunities. In 1924, Gaston Ramon (18861963) developed the method of chemical inactivation of bacterial toxins with formaldehyde and heat to produce toxoids of the pathogenic toxins of diphtheria and tetanus, producing safer vaccine antigens that retained their immunogenic potential. The Nobel Prize in Physiology or Medicine 1951 was awarded to Max Theiler (18991972) "for his discoveries concerning yellow fever and how to combat it.
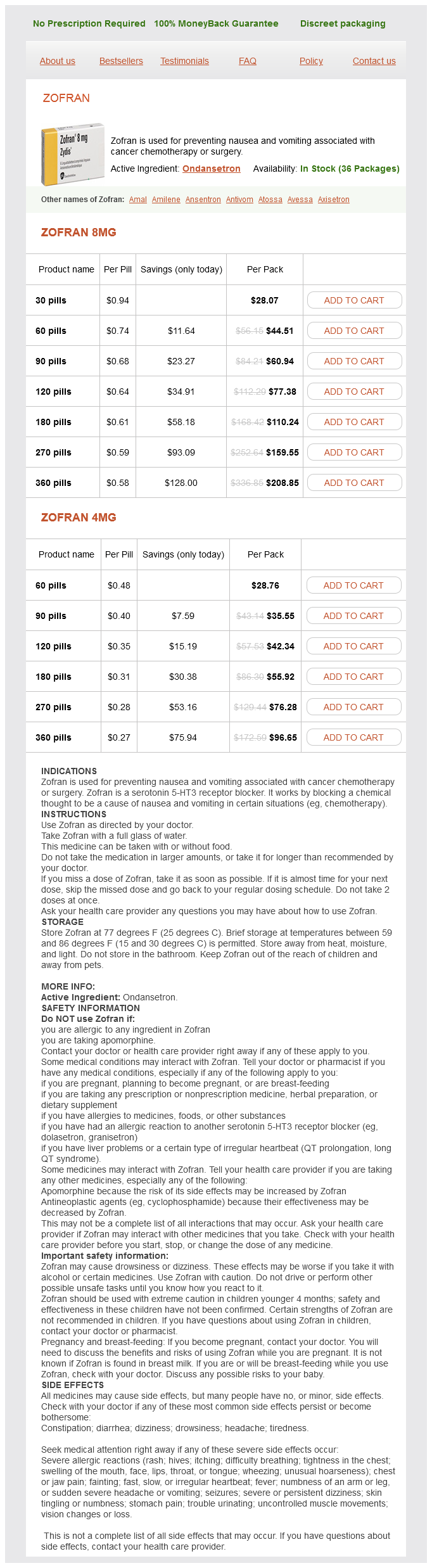
Zofran Dosage and Price
Zofran 8mg
- 30 pills - $28.07
- 60 pills - $44.51
- 90 pills - $60.94
- 120 pills - $77.38
- 180 pills - $110.24
- 270 pills - $159.55
- 360 pills - $208.85
Zofran 4mg
- 60 pills - $28.76
- 90 pills - $35.55
- 120 pills - $42.34
- 180 pills - $55.92
- 270 pills - $76.28
- 360 pills - $96.65
The diagnosis is established by immunofixation electrophoresis symptoms 3 dpo discount 8 mg zofran with mastercard, which shows that the abnormal protein consists only of gamma heavy chains without associated light chains. The serum protein electrophoretic pattern is usually normal, except for hypogammaglobulinemia. Although virtually all patients have multisystem amyloid deposition, it is not uncommon for a patient to present with evidence of mainly one organ involvement. Renal involvement occurs in approximately 70% of patients and most often presents as asymptomatic proteinuria or nephrotic syndrome. Cardiac involvement is seen in approximately 60% of patients and typically is characterized by thickening of the interventricular septum and ventricular wall. This can lead to systolic or diastolic dysfunction with symptoms of heart failure. Other manifestations that may be seen include sudden death or syncope due to arrhythmia or heart block and, rarely, angina or infarction due to accumulation of amyloid in the coronary arteries. Potential gastrointestinal manifestations include bleeding, gastroparesis, constipation, bacterial overgrowth, malabsorption, and intestinal pseudo-obstruction resulting from dysmotility. Symptoms of numbness, paresthesia, and pain are frequently noted, as in peripheral neuropathy of many other causes. Compression of peripheral nerves, especially the median nerve within the carpal tunnel, can cause more localized sensory changes. Symptoms of bowel or bladder dysfunction and findings of orthostatic hypotension may be due to autonomic nervous system damage. Arthropathy may be due to amyloid deposition in joints and surrounding structures. The "shoulder pad" sign is visible enlargement of the anterior shoulder due to fluid in the glenohumeral joint and/or amyloid infiltration of the synovial membrane and surrounding structures. Kidney or liver biopsy is positive for amyloid deposition in over 90% of cases; however, a high success rate can also be achieved by less invasive procedures, such as abdominal fat pad aspirate, rectal biopsy, bone marrow biopsy, or skin biopsy. There is, however, significant variability in median survival, depending on the nature, number, and extent of organ involvement. Median survival may range from 4 to 6 months in patients diagnosed at an advanced stage, to in excess of 5 years in patients with limited organ involvement. Two key prognostic factors include the presence and severity of cardiac involvement and the presence of concurrent myeloma. An alternative to mass spectrometry is to use immunoelectron microscopy, if available. The monoclonal light chain type is lambda in approximately 70% of cases, kappa in 25%, and biclonal in 5%. When serum and urine immunofixation electrophoresis is combined with serum free light chain ratio analysis, a monoclonal protein can be detected in virtually all cases. Less commonly, the bone marrow demonstrates overt myeloma or lymphoplasmacytic lymphoma. A clonal excess of plasma cells (lambda or kappa) can also be demonstrated by immunoperoxidase staining or flow cytometric analysis of specimens of involved bone marrow. These diseases are characterized by the deposition of immunoglobulin light or heavy chain fragments, leading to organ dysfunction. They are differentiated from light chain and heavy chain amyloidosis in that the light chain fragments do not have the necessary biochemical characteristics to form amyloid fibrils. The majority of patients present with hypertension, progressive renal dysfunction, anemia, and nephrotic syndrome with microhematuria. Tissue deposits of fragments of monoclonal light chains are commonly seen and can occur in a variety of organs, including the kidney, heart, liver, and small intestine. Routine electrophoretic techniques may not demonstrate a monoclonal protein in the serum or urine in some patients, but it may be detectable by serum free light chain analysis. To be included as a diagnostic criterion, the organ damage must be felt to be related to amyloid deposition and not to another common disease, such as diabetes or hypertension. Evidence that the amyloid is light chainrelated is established by direct examination of the amyloid using spectrometry-based proteomic analysis or immunoelectron microscopy. Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Clinical course and management of monoclonal gammopathy of undetermined significance. Serum free light chain ratio is an independent risk factor for progression in monoclonal gammopathy of undetermined significance. Revised International Staging System for Multiple Myeloma: A Report From International Myeloma Working Group. Criteria for diagnosis, staging, risk stratification and response assessment of multiple myeloma. Epidemiology, pathogenesis, clinical manifestations and diagnosis of Waldenstrom macroglobulinemia. Patient age <50 81 Concepts and Challenges in Organ Transplantation: Rejection, Immunosuppression, and Tolerance Kathryn J. Wood, Sushma Shankar, Joanna Hester, Fadi Issa the clinical era of transplantation began on December 23, 1954, when Dr. Joseph Murray and colleagues performed the first successful renal transplant on the genetically identical Herrick twins. However, this ground-breaking field within clinical immunology is not free of setbacks. Rejection of transplanted organs and tissues can result in devastating problems for the patient, and potent immunosuppression is associated with substantial comorbidity, including exposure to infection, malignancy, and cardiovascular risks that may be fatal. Theoretically, immunosuppression withdrawal and allograftspecific protection against host responses is the ultimate treatment to offer a transplant recipient. Although this is undoubtedly a challenging goal, it is being realized in defined subgroups of recipients.