General Information about Zyrtec
Zyrtec belongs to a class of medicine known as antihistamines. Its primary mechanism of motion is to dam the consequences of histamine, a chemical launched by the body during an allergic response. Histamine is answerable for causing the signs of hay fever and hives, similar to sneezing, itching, and inflammation. By blocking the consequences of histamine, Zyrtec helps to alleviate these symptoms and provide reduction to those who undergo from allergy symptoms.
Zyrtec, additionally recognized by its generic name cetirizine, is a popular antihistamine medicine used to treat hay fever and hives. Hay fever, also referred to as allergic rhinitis, is a typical situation by which the immune system overreacts to allergens in the air, causing signs corresponding to sneezing, itching, and a runny nostril. Hives, also referred to as urticaria, is a skin situation characterised by itchy, raised welts on the pores and skin. Zyrtec is a highly efficient treatment in relieving the symptoms of these circumstances and has been extensively used for a few years.
While Zyrtec is usually well-tolerated, some folks might experience gentle side effects such as drowsiness, dry mouth, and headache. These unwanted effects are usually temporary and can subside after a few days of taking the medicine. However, if they persist or turn into severe, it is very important converse to a healthcare provider.
One of the primary benefits of Zyrtec is its long-lasting effects. It is a once-a-day medicine, that means that a single dose can present aid from signs for the whole day. This is beneficial for people who lead busy lives and don't have time to take multiple doses all through the day. Zyrtec also has a fast onset of motion, with many people experiencing aid from symptoms inside 20-30 minutes after taking the medicine.
In rare cases, Zyrtec might interact with other drugs, similar to sedatives, tranquilizers, and certain antidepressants. It is crucial to inform your physician about all of the medicines you might be at present taking earlier than beginning Zyrtec.
Zyrtec is on the market in multiple varieties, including tablets, chewable tablets, and syrup, making it easy for people of all ages to take. The really helpful dosage for adults and kids over the age of 6 is 10mg once every day, while youngsters between the ages of 2-6 should take 5mg once a day. Zyrtec can be obtainable over-the-counter, making it simply accessible for many who don't have a prescription from their physician.
Zyrtec can be protected for use in being pregnant and while breastfeeding. However, as with any treatment, it is essential to consult with a health care provider before taking Zyrtec throughout being pregnant or whereas breastfeeding to make sure it's protected for both the mother and the infant.
In conclusion, Zyrtec is a extremely effective treatment for the therapy of hay fever and hives. With its long-lasting results, quick onset of action, and numerous types of administration, it's a convenient and popular choice for these affected by allergic reactions. If you expertise symptoms of hay fever or hives, consult together with your healthcare provider to see if Zyrtec may be an acceptable treatment option for you.
They serve as weapons in many mammals but became reduced in the course of human evolution until they now project barely beyond the other teeth allergy forecast las vegas buy zyrtec canada. The premolars and molars have relatively broad, lumpy surfaces adapted for crushing, shredding, and grinding; they are often informally called the grinders. Each tooth is embedded in a socket called an alveolus, forming a joint called a gomphosis between the tooth and bone (fig. This anchors the tooth firmly in the alveolus but allows for slight movement under the stress of chewing. The ligament is innervated by proprioceptive nerve fibers that enable one to sense tooth movements and bite force. Regions of a tooth are defined by their relationship to the gingiva: the crown is the portion above the gum attachment; the root is the portion below the gum, embedded in alveolar bone; and the neck is the point where the crown, root, and gum meet. The hygiene of this sulcus is especially important to dental health (see Deeper Insight 25. With some variation, the incisors and canines have a single root; the premolars have one or two roots; the first and second molars have two to three roots; and in the third molar, the roots are usually fused into one. These acids dissolve the minerals of enamel and dentin, and the bacteria enzymatically digest the collagen and other organic components. This requires either extraction of the tooth or root canal therapy, in which the pulp is removed and replaced with inert material. Calculus in the gingival sulcus wedges the tooth and gum apart and allows bacterial invasion of the sulcus. In some cases, bacteria spread from the sulcus into the alveolar bone and begin to dissolve it, producing periodontal disease. About 86% of people over age 70 have some degree of periodontal disease and many suffer tooth loss as a result. This grinds and tears food more effectively than if the occlusal surfaces were flat. Twenty deciduous teeth (milk teeth or baby teeth) erupt from the ages of 6 to 30 months, beginning with the incisors (fig. Over the course of human evolution, the face became flatter and the jaws shorter, leaving little room for the third molars. Thus, they often remain below the gum and become impacted-so crowded against neighboring teeth and bone that they cannot erupt. Mastication requires little thought because food stimulates oral receptors that trigger an automatic chewing reflex. The tongue, buccinator, and orbicularis oris muscles manipulate food and push it between the teeth. The masseter and temporalis muscles produce the up-and-down crushing action of the teeth, and the lateral and medial pterygoid muscles and masseters produce side-to-side grinding action (see fig. Most of a tooth consists of hard yellowish tissue called dentin, covered with enamel in the crown and cement in the root. Dentin and cement are living connective tissues with cells or cell processes embedded in a calcified matrix. Cells of the cement (cementocytes) are scattered more or less randomly and occupy tiny cavities similar to the lacunae of bone. Cells of the dentin (odontoblasts) line the pulp cavity and have slender processes that travel through tiny parallel tunnels in the dentin. Enamel is not a tissue but a cell-free secretion produced before the tooth erupts above the gum. Damaged dentin and cement can regenerate, but damaged enamel cannot-it must be artificially repaired. Internally, a tooth has a dilated pulp cavity in the crown and a narrow root canal in the lower root. These spaces are occupied by pulp-a mass of loose connective tissue, blood and lymphatic vessels, and nerves. These nerves and vessels enter the tooth through a pore, the apical foramen, at the basal end of each root canal. The occlusal surfaces of the premolars and molars have rounded bumps called cusps-two on each of the premolars and four to five on the molars. Cusps of the upper and lower premolars and molars mesh when the jaws are closed and slide over each other as the jaw makes lateral chewing motions. This dissection shows erupted deciduous teeth and, deep to them and marked with asterisks, the permanent teeth waiting to erupt. Sublingual ducts Masseter muscle the Salivary Glands There are two kinds of salivary glands, intrinsic and extrinsic. The intrinsic (minor) salivary glands are an indefinite number of small glands dispersed amid the other oral tissues- lingual glands in the tongue, labial glands on the inside of the lips, palatine glands of the palate, and buccal glands on the inside of the cheeks. The extrinsic (major) salivary glands are three pairs of larger, more discrete organs located outside of the oral mucosa. The secretory acini at the twig ends of the tree are in some cases purely mucous, in others purely serous, and in mixed acini, composed of both mucous and serous cells (fig. The parotid duct passes superficially over the masseter muscle, pierces the buccinator muscle, and opens into the mouth opposite the second upper molar tooth. The submandibular glands are located halfway along the body of the mandible, medial to its margin, just deep to the mylohyoid muscle. The submandibular duct empties into the mouth at a papilla on the side of the lingual frenulum, near the lower central incisors. They have multiple ducts that empty into the mouth posterior to the papillae of the submandibular ducts.
As this entity is still relatively new allergy shots for yellow jackets zyrtec 5 mg purchase line, further studies are needed to better delineate its features [10]. This is unlike classical vitiligo, where cutaneous depigmentation is the predominant clinical feature and hairs are usually spared. It is believed that in the setting of genetically predisposed individuals, melanocyte-intrinsic abnormalities coupled with accumulated oxidative stress result in cellular damage, loss of the hair follicle immune privilege, immune activation, and exposure of a unique follicular melanocyte antigen leading to loss of hair pigmentation. In this condition, melanocytes are absent in the hair follicle, whereas in classical vitiligo without leukotrichia, melanocytes are not completely absent from the follicular unit [13,14]. The presence of an intermediary or transitional zone between affected and normal skin suggests a centrifugal spread of hypomelanosis. This intermediate layer is also sometimes referred to as the "intermediate tan zone," while the entire pattern has also been referred to as "cockade-like" [6]. Of note, trichrome vitiligo tends to be found in photoprotected areas such as the trunk, abdomen, back, and buttocks. Histologically, lesions of trichrome vitiligo are characterized by the presence of an inflammatory infiltrate and vacuolar degeneration of the basal layer, which is especially accentuated around the melanocytes [15]. This was followed by development of depigmented patches on the scalp, trunk, and limbs. In such patients, this is a sign of improvement, where the additional brown color is present due to perifollicular or marginal repigmentation. Interestingly, pentachrome vitiligo has been described, where there are five shades of colors, namely white, tan, medium brown (unaffected skin), dark brown, and black. She presented with areas of complete depigmentation over the face, trunk, and extremities, as well as hypopigmented tan macules and patches between depigmented areas and normal medium brown skin. Strikingly, this patient also had dark brown areas over the buttocks, toes, and fingers, and patches of black skin in the intragluteal folds and elbows. Histologically, the areas of depigmentation demonstrated complete loss of melanin while the hypopigmented tan areas had a corresponding decreased amount of epidermal melanin and fewer melanocytes. It is likely that the epidermal and follicular melanocytes demonstrate different antigenic profiles, and so represent two separate reserves of slightly differing melanocytes, thereby explaining how this subtype of vitiligo arises. In patients with follicular vitiligo, the absence of follicular melanocytes and their precursors unfortunately confers a poorer prognosis and treatment response [12]. The center is completely depigmented and achromic, followed by a zone of intermediate hypopigmentation, which is then surrounded by unaffected and clearly demarcated normal skin in the periphery. On closer inspection, confetti-like depigmented macules can also be seen along the borders of several patches. Sparse lymphocytic infiltrate and melanophages were observed in the biopsies taken from both hypo- and hyperpigmented areas [16]. This patient subsequently progressed into widespread spontaneous depigmentation within 1 year of presentation. What remains unusual about this case is the presence of markedly hyperpigmented areas with increased melanocytes, a feature that still remains unexplained. The nonuniformity in size of the macules, from being pinpoint to several millimeters in diameter, explains the name "confetti-like. Early pilot studies indicate that this may constitute a sign of active and spreading inflammation and may herald rapidly progressive disease [17]. Histologically, a lymphocytic infiltrate can be seen at the dermo- epidermal junction together with a lack of melanocytes. The presence of this feature also indicates a greater likelihood of rapidly progressive disease [18]. Chemical leukoderma is a close differential, and a detailed history of chemical exposure is required. This pattern of hypopigmentation may also arise separately as a result of phototherapy or after repeated pigment laser treatment for melasma [19]. Koebnerization has been reported with this rare variant, which can occur at any age and without gender predilection [21]. The lesions tend to involve extensive body surface areas and are generally considered progressive and unstable. Of note, concomitant inflammatory and clinically non-inflammatory patches may occur in the same patient [22]. Mycosis fungoides is an important differential which cannot be missed, as this condition can sometimes present with hypopigmented lesions which have an inflammatory edge [24]. Histologically, a biopsy from the inflammatory border shows psoriasiform hyperplasia and parakeratosis, corresponding to the scaling seen clinically [21]. There is a mononuclear inflammatory infiltrate located perivascularly and often in a lichenoid pattern, with reports of degeneration of melanocytes and basal keratinocytes [25]. This entity lends support to the theory that vitiligo is an inflammatory disorder. In fact, depigmentation in vitiligo has been observed to pass through two stages in patients with skin of color. In stage 1, the initial affected area may be urticarial or have a dermatitis-like morphology with underlying erythema. This subsequently fades into a milky or chalk-white color and becomes well demarcated from surrounding normal skin as it enters stage 2 [28]. Histologically, stage 1 frequently demonstrates an inflammatory infiltrate, especially in the marginal areas, and these inflammatory cells gather in small foci surrounding melanocytes. In some cases, the inflammatory response may be large enough, resulting in extensive spongiosis and keratinocyte degeneration. This corresponds to the varied inflammatory clinical morphologies seen in stage 1. In stage 2, the inflammatory infiltrate is less common and, when present, much less intense as compared to stage 1. In patients with inflammatory vitiligo, treatment with topical corticosteroids and calcineurin inhibitors leads to improvement of the erythema at the border, albeit without repigmentation.
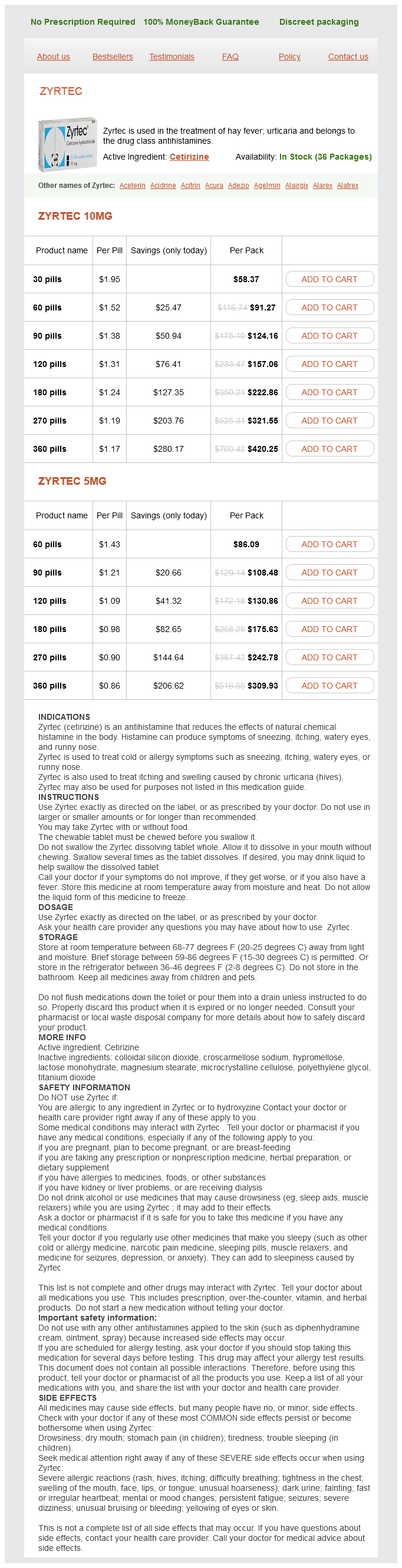
Zyrtec Dosage and Price
Zyrtec 10mg
- 30 pills - $58.37
- 60 pills - $91.27
- 90 pills - $124.16
- 120 pills - $157.06
- 180 pills - $222.86
- 270 pills - $321.55
- 360 pills - $420.25
Zyrtec 5mg
- 60 pills - $86.09
- 90 pills - $108.48
- 120 pills - $130.86
- 180 pills - $175.63
- 270 pills - $242.78
- 360 pills - $309.93
In contrast allergy forecast virginia beach discount zyrtec 10 mg on-line, two fatalities showing only discrete signs of injury on external examination were not recognized as homicides at the scene. Four corpses had merely been deposited in the bathtub, and waterlogging had not actually influenced the lethal outcome. Four homicides were committed partly or completely in the bathtub (drowning, strangulation, ligature strangulation with the tube of the shower). In two cases the scenario raised the question of whether the victim had been put into the bathtub after manual strangulation to ensure death by electrocution. Case 2 In the second case, a 37-year-old woman was found dead in her bathtub with her mouth and nose submerged in water and abundant white foam escaping from the mouth. In addition, haemorrhages of the skin were found in the sacral region and over both elbows as well as haemorrhages of the soft tissues covering the thoracic and lumbar spinal column and the left clavicula. The lungs were large and bulky and on cut sections had a brick-red appearance with large quantities of foamy oedema fluid flowing from the cut surfaces. Case 1 In this case, a 32-year-old woman was found dead by her husband in the bathtub, lying undressed, face down, with her mouth and nose beneath the surface of the water. On the floor of the living room a pool of blood was encountered with a trace of dragging leading in the direction of the bathroom. The autopsy revealed a ligature mark of the neck, corresponding paleness of the mucous membrane of the gullet and multiple petechiae of the conjunctivae. In addition, a deep incised wound of the throat was found, but there were no signs of blood aspiration, air embolism or marked anaemia of the internal organs due to haemorrhage. In court the perpetrator confessed that, in the course of a fight with a sexual background, he had first strangled the woman with the electric cord, inflicted the incised wound of the neck and then submerged the corpse in the bathtub. The analysis of our autopsy material, however, is intended to give a survey of the entire spectrum encountered and to elucidate the problems in establishing the diagnosis of cause and manner of death apart from drowning and electrocution. In our material young women aged 2040 years make up most of the victims of a homicide found in the bathtub. This is in good agreement with the data from the literature summarized above (sex: 21 females, 4 males; age: 4 children, 11 adults aged 2040 years, 6 adults >40 years). In our material comprising only homicides, autopsy revealed evidence of aspirating, respectively swallowing water in 36 per cent of the cases. In every case they indicated that the victim was still alive when entering or being put into the bathtub. In one case the autopsy findings of drowning brought about the suspicion of homicide, and in two cases drowning was the cause of death. In comparison, analysis of the literature cited in the tables above renders the following distribution: 14 by strangulation, 10 by drowning, 6 by electrocution, 5 by blunt force and 5 by sharp force. The lack of homicidal electrocution in our material is due to the fact that this cause of death was not proved beyond doubt in any case. The problems of verifying lethal electrocution and of distinguishing between suicide, accident and homicide under the conditions of waterlogging are well known [2931,36,52,66,82,115,134,135,141,152154,179,181]. Although findings of severe miscellaneous violence allowed the unequivocal diagnosis of homicide in eight cases, one case of drowning and one case of manual strangulation were not recognized before the autopsy (possible reasons are discussed below). Case 3 In the third case, a 55-year-old woman was found by her son face down submerged in her bathtub, with her mouth and nose beneath the water. Faint haemorrhages and scratches of the skin and the neck recognized on external examination at the scene were supposed to be related to a necklace. Looking at the case reports, in Case 1 the autopsy findings were in good agreement with the later confession of the perpetrator. There is no doubt that, referring to Trübner and Püschel [169], the scenario and autopsy findings of this fatality were highly indicative of the manner and cause of death. According to the classification of Kruger and colleagues [90], the corpse had merely been deposited in the bathtub and this was of no importance for the occurrence of death. In another case the perpetrator explained that he had stabbed his wife and then given her a shower to remove the traces [90]. In a further case in our material, the perpetrators described stabbing their victim and then submerging them in the bathtub to ensure death. Considering the circumstances at the scene, the severe injuries of the neck as well as the haemorrhages in the skin and the soft tissues of the neck may have been related to a blunt force pushing the body against the front side of the bathtub, and they leave no doubt as to the diagnosis of homicide. Particularly in cases of ligature or manual strangulation, the police and the forensic pathologist may encounter serious difficulties in establishing the cause of death (as observed by Spitz [161]). Mueller [121] has emphasized that abrasions of the skin due to manual strangulation or other causes may be barely visible on wet skin but become more obvious some hours later. In particular, the surface pattern reflecting the nature of the ligature may disappear. Bode and Kampmann [28] succeeded in making an experimentally produced strangulation furrow completely disappear by combined treatment with ointments and exposure to water. These observations and experimental results underline the belief that a thorough autopsy should be carried out on every suspicious fatality in the bathtub, even if first examination at the scene does not reveal any severe injury. About 65 per cent of the child homicides were committed by the mother in the parental flat, predominantly in the early hours of the evening during the weekend. The modes of death were 9 blunt injury, 6 sharp violence, 6 strangulation, 3 smothering, 2 drowning, 2 gunshot and 5 neglect (starvation) (Table 18. The defenseless, helpless and immobile condition of the infant particularly favours a homicide by manual assault, smothering or neglect (starvation).